
Barriers to Water and Sanitation Safety Plans in Rural Areas of South Africa—A Case Study in the Vhembe District, Limpopo Province


 ,
, 
 ,
,  , and
, and
Abstract
:1. Introduction
2. Methodology
Ethical Approval
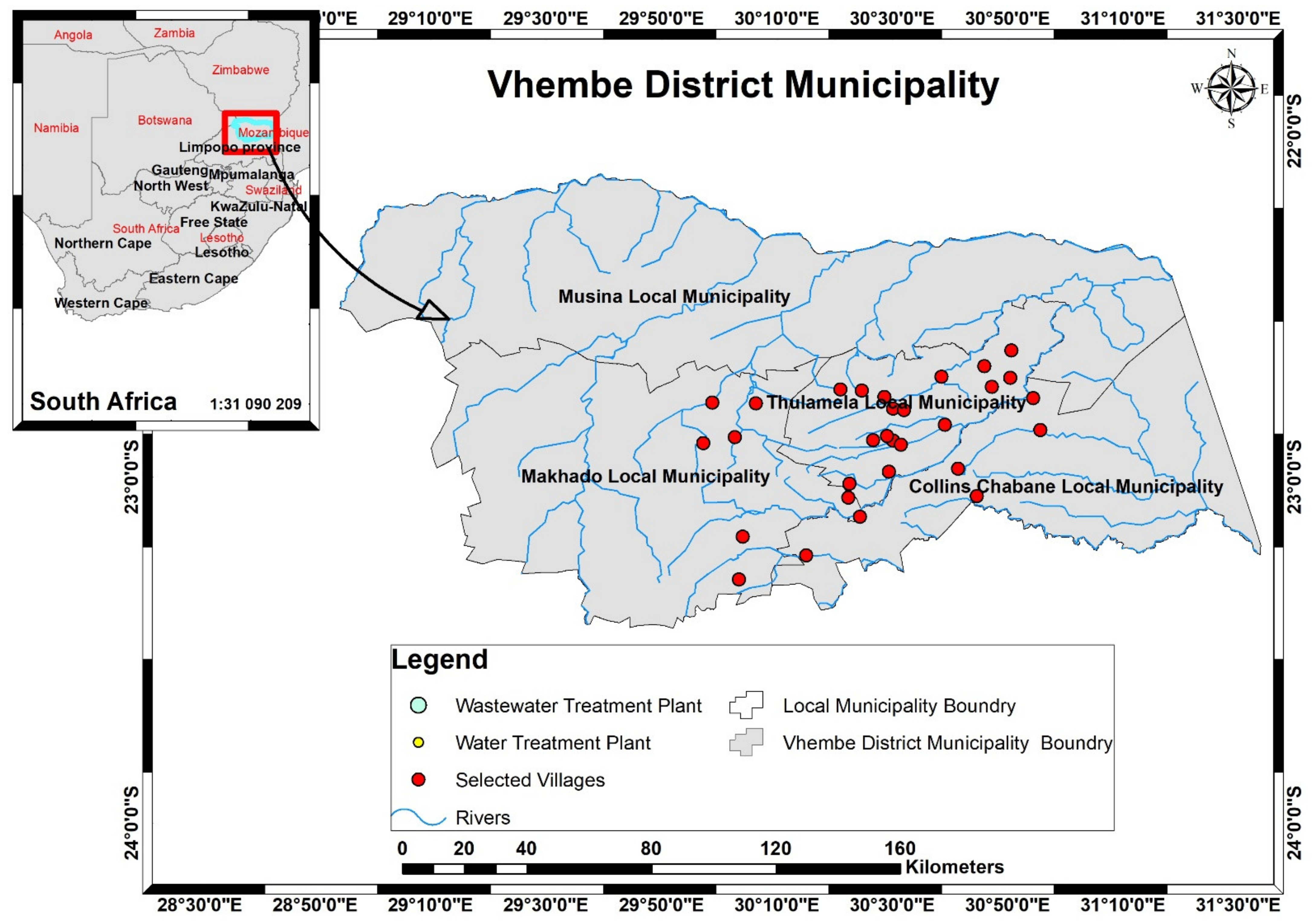
3. Description of the Study Area
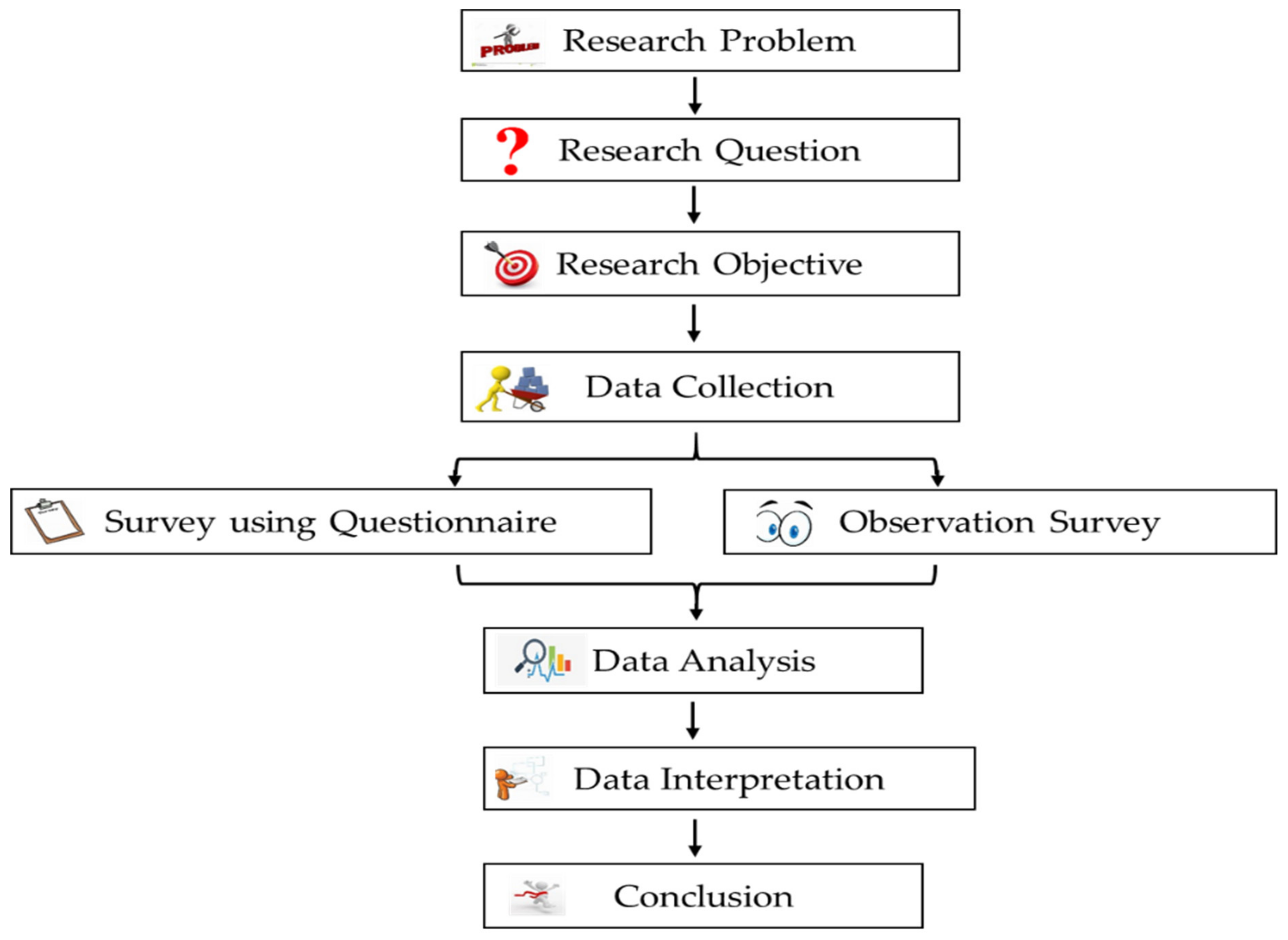
4. Data Collection
5. Statistical Analysis
6. Results
6.1. Socio-Demographic Data
6.2. Water, Sanitation, and Hygiene (WASH) Data in Vhembe District Municipality
6.3. Water Treatment Plants
6.3.1. Potable Water
6.3.2. Wastewater
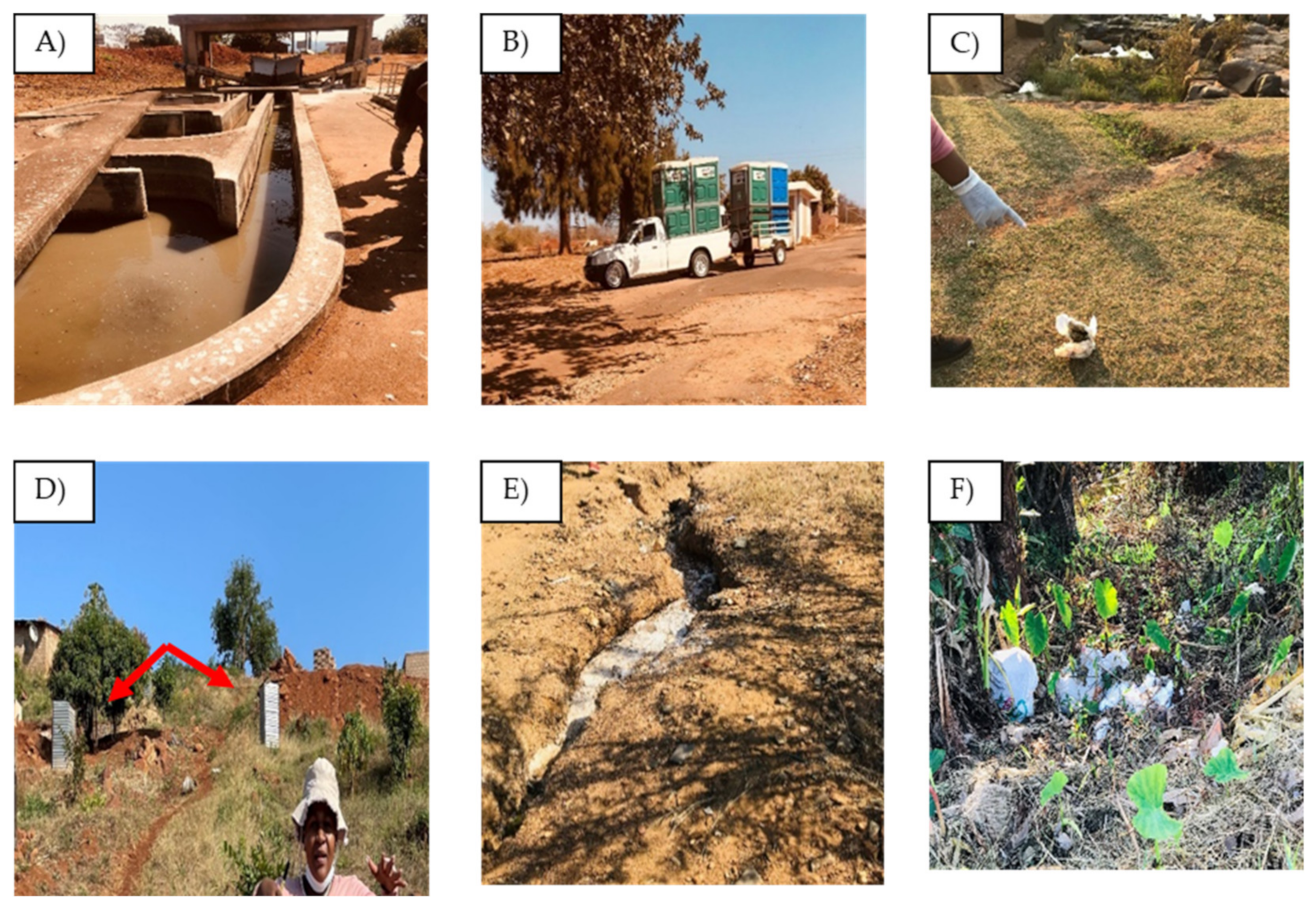
6.3.3. Main Activities Observed around Water Sources
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Freeman, M.C.; Clasen, T.; Dreibelbis, R.; Saboori, S.; Greene, L.E.; Brumback, B.; Muga, R.; Rheingans, R. The impact of a school-based water supply and treatment, hygiene, and sanitation programme on pupil diarrhoea: A cluster-randomized trial. Epidemiol. Infect. 2014, 142, 340–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO (World Health Organization). 2020. Available online: https://www.who.int/publications-detail/recommendations-to-member-states-to-improve-hand-hygiene-practices-to-help-prevent-the-transmission-of-the-covid-19-virus (accessed on 20 August 2021).
- Hara, M.; Ncube, B.; Sibanda, D. Water and Sanitation in the Face of COVID-19 in Cape Town’s Townships and Informal Settlements. 2020. Available online: https://www.plaas.org.za/water-and-sanitation-in-the-face-of-covid-19-in-cape-towns-townships-and-informal-settlements/ (accessed on 31 August 2021).
- UN (United Nation). 2020. Available online: https://www.un.org/development/desa/dpad/publication/un-desa-policy-brief-86-the-long-term-impact-of-covid-19-on-poverty/ (accessed on 20 August 2021).
- Monyane, M.; Ramcharan-Kotze, C.; Naidoo, V.; Reddick, J.; Mpofu, A.; Levin, S. A Case for Water and Sanitation in South Africa’s Post-Lockdown Economic Recovery Stimulus Package. 2020. Available online: https://www.tips.org.za/images/TIPS_Policy_Brief_A_case_for_water_and_in_South_Africas_post_lockdown_stpdf.pdf (accessed on 28 August 2021).
- World Health Organization; UNICEF. Progress on Sanitation and Drinking-Water: 2010 Update; World Health Organisation: Geneva, Switzerland, 2010; Available online: https://apps.who.int/iris/handle/10665/44272 (accessed on 4 August 2021).
- Neves-Silva, P.; Heller, L. The right to water and sanitation as a tool for health promotion of vulnerable groups. Ciencia Saude Coletiva 2016, 21, 1861–1870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rankoana, S.; Mothiba, T. Water scarcity and women’s health: A case of Sagole community in Mutale Local Municipality, Vhembe District of Limpopo Province, South Africa. Afr. J. Phys. Health Educ. Recreat. Dance 2015, 4, 738–744. [Google Scholar]
- World Bank Group. Central African Republic: Priorities for Ending Poverty and Boosting Shared Prosperity. 2019. Available online: https://openknowledge.worldbank.org/handle/10986/23099 (accessed on 7 August 2021).
- Bain, R.; Wright, J.; Yang, H.; Gundry, S.; Pedley, S.; Bartram, J. Improved but not necessarily safe: Water access and the Millennium Development Goals. In Global Water: Issues and Insights; ANU Press: Acton, ACT, Australia, 2014. [Google Scholar]
- Cabral, J.P. Water microbiology. Bacterial pathogens and water. Int. J. Environ. Res. Public Health 2010, 7, 3657–3703. [Google Scholar] [CrossRef] [PubMed]
- Nthunya, L.N.; Maifadi, S.; Mamba, B.B.; Verliefde, A.R.; Mhlanga, S.D. Spectroscopic Determination of Water Salinity in Brackish Surface Water in Nandoni Dam, at Vhembe District, Limpopo Province, South Africa. Water 2018, 10, 990. [Google Scholar] [CrossRef] [Green Version]
- Jones, H.; Fisher, J.; Reed, R. Water and sanitation for all in low-income countries. Proc. Inst. Civ. Eng. Munic. Eng. 2012, 165, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Pantaleo, P.A. Risks of Sanitation Facilities to Groundwater Pollution in Babati Town, Tanzania. Master’s Thesis, Nelson Mandela African Institution of Science and Technology, Arusha, Tanzania, March 2019. [Google Scholar]
- Momba, M.N.; Mnqumevu, B.V. Detection of faecal coliform bacteria and heterotrophic plate count bacteria attached to household containers during the storage of drinking water in rural communities. In Proceedings of the WISA Annual Conference, Sun City, South Africa, 28 May–1 June 2000. [Google Scholar]
- Momba, M.N.; Malakate, V.K.; Theron, J. Abundance of pathogenic Escherichia coli, Salmonella typhimurium and Vibrio cholerae in Nkonkobe drinking water sources. J. Water Health 2006, 4, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Mpenyana-Monyatsi, L.; Onyango, M.S.; Momba, M.B. Groundwater quality in a South African rural community: A possible threat to public health. Pol. J. Environ. Stud. 2012, 21, 1349–1358. [Google Scholar]
- Mackintosh, G.; Colvin, C. Failure of rural schemes in South Africa to provide potable water. Environ. Geol. 2003, 44, 101–105. [Google Scholar] [CrossRef]
- World Health Organization. Progress on Sanitation and Drinking Water—2015 Update and MDG Assessment. 2015. Available online: https://apps.who.int/iris/handle/10665/177752 (accessed on 15 August 2021).
- Samwel, M. Developing a Water and Sanitation Safety Plan in a Rural Community. How to Accomplish a Water and Sanitation Safety Plan? WECF Compendium—Part A Compendium; Women in Europe for a Common Future: Bonn, Germany, 2014. [Google Scholar]
- WHO (World Health Organization). Guidelines for Drinking-Water Quality (Volume 1). 2004. Available online: http://www.who.int/water_sanitation_health/dwq/gdwq3rev/en/index.html (accessed on 2 July 2021).
- UNESCO (United Nations Educational, Scientific and Cultural Organization). Available online: https://unevoc.unesco.org/home/Skills%20development%20for%20the%20water%20and%20sanitation%20sector%20in%20Vietnam (accessed on 2 July 2021).
- Sibiya, J.E.; Gumbo, J.R. Knowledge, attitude and practices (KAP) survey on water, sanitation and hygiene in selected schools in Vhembe District, Limpopo, South Africa. Int. J. Environ. Res. Public Health 2013, 10, 2282–2295. [Google Scholar] [CrossRef] [PubMed]
- Stats SA (Statistics South Africa). Available online: http://www.statssa.gov.za/?page_id=964 (accessed on 24 July 2021).
- Dupas, P.; Nhlema, B.; Wagner, Z.; Wolf, A.; Wroe, E. Expanding Access to Clean Water for the Rural Poor: Experimental Evidence from Malawi (No. w27570); National Bureau of Economic Research: Cambridge, MA, USA, 2020. [Google Scholar]
- Key, J.D. Development of a Small-Scale Electro-Chlorination System for Rural Water Supplies. Ph.D. Thesis, University of Western Cape, Cape Town, South Africa, 2010. [Google Scholar]
- Moropeng, R.C.; Momba, M.N.B. Assessing the Sustainability and Acceptance Rate of Cost-Effective Household Water Treatment Systems in Rural Communities of Makwane Village, South Africa. Crystals 2020, 10, 872. [Google Scholar] [CrossRef]
- Nthunya, L.N.; Khumalo, N.P.; Verliefde, A.R.; Mamba, B.B.; Mhlanga, S.D. Quantitative analysis of phenols and PAHs in the Nandoni Dam in Limpopo Province, South Africa: A preliminary study for dam water quality management. Phys. Chem. Earth Parts A/B/C 2019, 112, 228–236. [Google Scholar] [CrossRef]
- Mnisi, R. An Assessment of the Water and Sanitation Problems in New Forest, Bushbuckridge Local Municipality, South Africa. Master’s Thesis, Free State University, Bloemfontein, South Africa, 2011. [Google Scholar]
- Khabo-Mmekoa, C.M.N.; Momba, M.N.B. The Impact of Social Disparities on Microbiological Quality of Drinking Water Supply in Ugu District Municipality of Kwazulu-Natal Province, South Africa. Int. J. Environ. Res. Public Health 2019, 16, 2972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Government Gazette. Republic of South Africa, Regulation Gazette No. 7079, Volume 432. 2001. Available online: https://ec.europa.eu/echo/files/evaluation/watsan2005/annex_files/SA/SA1%20-%20South%20Africa%20Watsan%20Regulations.pdf (accessed on 30 August 2021).
- Mnisi, N. COVID-19 Challenges and Opportunities for Water Sanitation and Hygiene Sector. 2020. Available online: https://www.politicsweb.co.za/opinion/covid19-challenges-and-opportunities-for-water-san (accessed on 28 August 2021).
- Angoua, E.L.E.; Dongo, K.; Templeton, M.R.; Zinsstag, J.; Bonfoh, B. Barriers to access improved water and sanitation in poor peri-urban settlements of Abidjan, Côte d’Ivoire. PLoS ONE 2018, 13, e0202928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oloruntoba, E.O.; Folarin, T.B.; Ayede, A.I. Hygiene and sanitation risk factors of diarrhoeal disease among under-five children in Ibadan, Nigeria. Afr. Health Sci. 2014, 14, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Cloutman-Green, E.; Kalaycioglu, O.; Wojani, H.; Hartley, J.C.; Guillas, S.; Malone, D.; Gant, V.; Grey, C.; Klein, N. The important role of sink location in handwashing compliance and microbial sink contamination. Am. J. Infect. Control. 2014, 42, 554–555. [Google Scholar] [CrossRef] [PubMed]
- Mwelase, L.T. Water supply interruptions in Umzinto Water System: Ugu District, South Africa. Int. J. Water Resour. Environ. Eng. 2021, 13, 135–153. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics of Household’s Respondents | Local Municipalities | ||||||
|---|---|---|---|---|---|---|---|
| Thulamela | Collins-Chabane | Makhado | |||||
| Number | Percentage | Number | Percentage | Number | Percentage | ||
| Age groups | 0–5 | 263 | 12.5% | 320 | 16.0% | 230 | 12.2% |
| 6–15 | 386 | 18.4% | 396 | 19.8% | 358 | 19.0% | |
| 16–25 | 400 | 19.1% | 350 | 17.5% | 345 | 18.3% | |
| 26–55 | 691 | 32.9% | 653 | 32.7% | 686 | 36.3% | |
| ≥56 | 360 | 17.1% | 280 | 14.0% | 269 | 14.3% | |
| n = 2100 | n = 1999 | n = 1888 | |||||
| Educational level | No schooling | 15 | 1.6% | 31 | 3.9% | 20 | 2.0% |
| Primary | 88 | 8.0% | 48 | 6.0% | 64 | 6.5% | |
| Secondary | 135 | 12.2% | 87 | 10.9% | 141 | 14.4% | |
| Matric | 607 | 55.0% | 469 | 58.8% | 501 | 51.1% | |
| Tertiary | 258 | 23.4% | 163 | 20.4% | 254 | 25.9% | |
| n = 1103 | n = 798 | n = 980 | |||||
| Number of employed individual(s) in the household | 0 | 228 | 44.1% | 188 | 45.0% | 152 | 35.9% |
| 1 | 190 | 36.7% | 134 | 32.1% | 167 | 39.4% | |
| 2 | 82 | 15.9% | 79 | 18.9% | 78 | 18.2% | |
| 3 | 16 | 3.1% | 14 | 3.4% | 24 | 5.7% | |
| ≥4 | 1 | 0.2% | 3 | 0.7% | 3 | 0.7% | |
| n = 517 | n = 418 | n = 424 | |||||
| Monthly salary distribution | ≤ZAR 5000 | 1149 | 91.6% | 240 | 43.0% | 199 | 6.7% |
| ZAR 5000–ZAR 10,000 | 83 | 6.6% | 303 | 54.3% | 73 | 24.6% | |
| ≥ZAR 10,000 | 23 | 1.8% | 15 | 2.7% | 25 | 8.4% | |
| n = 1255 | n = 588 | n = 279 | |||||
| Illnesses affecting VDM population | Diarrhoea | 93 | 17.9% | 71 | 16.1% | 45 | 10.6% |
| Trachoma | 8 | 1.5% | 7 | 1.6% | 9 | 2.1% | |
| Body lice | 3 | 0.6% | 0 | 0% | 0 | 0% | |
| Rash | 21 | 4.0% | 21 | 4.8% | 2 | 0.5% | |
| None | 395 | 76.0% | 343 | 77.6% | 368 | 86.4% | |
| n = 520 | n = 442 | n = 426 | |||||
| Does diarrhoeal frequency occur | Yes | 18 | 12.3% | 430 | 7.6% | 418 | 7.8% |
| No | 502 | 87.7% | 430 | 92.4% | 418 | 92.2% | |
| n = 520 | n = 442 | n = 426 | |||||
| Characteristics of Household’s Respondents | Local Municipalities | ||||||
|---|---|---|---|---|---|---|---|
| Thulamela | Collins-Chabane | Makhado | |||||
| Number | Percentage | Number | Percentage | Number | Percentage | ||
| Main water sources | Communal tap * | 223 | 42.8% | 178 | 40.2% | 128 | 30.1% |
| Tap in dwelling * | 252 | 48.4% | 252 | 57.1% | 239 | 56.2% | |
| Rain | 9 | 1.7% | 0 | 0% | 0 | 0% | |
| Borehole | 21 | 4.1% | 0 | 0% | 48 | 11.3% | |
| Spring | 4 | 0.8% | 3 | 0.7% | 10 | 2.4% | |
| Truck-tanker * | 0 | 0% | 0 | 0% | 0 | 0% | |
| River | 11 | 2.1% | 9 | 2.0% | 1 | 0.2% | |
| Bottled * | 0 | 0% | 0 | 0% | 0 | 0% | |
| n = 520 | n = 442 | n = 426 | |||||
| Knowledge of household water treatment methods | Do not know | 193 | 37.1% | 191 | 45.3% | 188 | 44.3% |
| Bleaching/Chlorination | 105 | 20.2% | 103 | 24.5% | 105 | 24.8% | |
| Boiling | 153 | 29.4% | 100 | 23.8% | 106 | 24.8% | |
| Salting | 13 | 2.5% | 4 | 1.0% | 1 | 0.2% | |
| Bleaching/Boiling/Salting | 11 | 8.7% | 1 | 5.2% | 0 | 0.0% | |
| Other | 45 | 2.1% | 45 | 0.2 | 25 | 5.9 | |
| n = 520 | n = 421 | n = 425 | |||||
| Water treatment methods usage in households | Do not use | 375 | 72.2% | 374 | 72.1% | 393 | 75.6% |
| In use | 144 | 27.8% | 145 | 27.9% | 126 | 24.4% | |
| n = 520 | n = 442 | n = 426 | |||||
| Sanitation facilities used | Pit | 366 | 70.4% | 268 | 60.6% | 288 | 67.6% |
| Pit with concrete slab | 122 | 23.5% | 127 | 28.7% | 91 | 21.4% | |
| Flush septic | 16 | 3.1% | 1 | 0.0% | 36 | 8.5% | |
| VIP | 1 | 0.0% | 1 | 0.0% | 1 | 0.0% | |
| Open defecation | 7 | 1.3% | 16 | 3.6% | 9 | 2.1% | |
| Neighbours | 7 | 1.3% | 5 | 1.1% | 0 | 0% | |
| n = 520 | n = 442 | n = 426 | |||||
| Who built sanitation facility | Municipality | 181 | 34.9% | 176 | 39.8% | 116 | 31.2% |
| household member | 179 | 34.5% | 109 | 24.7% | 69 | 18.5% | |
| Hired personnel | 139 | 26.2% | 122 | 27.6% | 178 | 47.8% | |
| None/no toilet | 23 | 4.2% | 35 | 7.9% | 9 | 2.4% | |
| n = 519 | n = 442 | n = 372 | |||||
| Is the sanitation facility still in good condition | Yes | 469 | 90% | 380 | 86% | 363 | 85% |
| No | 50 | 10% | 62 | 14% | 63 | 15% | |
| n = 519 | n = 442 | n = 426 | |||||
| Availability of hand-washing basin | Yes | 47 | 9.2% | 54 | 14.9% | 22 | 5.7% |
| No | 464 | 90.8% | 363 | 87.1% | 412 | 94.9% | |
| n = 511 | n = 417 | n = 434 | |||||
| Proper hygiene practice in study population | Yes | 431 | 82.9% | 403 | 91.2% | 381 | 89.4% |
| No | 71 | 13.7% | 28 | 6.3% | 36 | 8.5% | |
| Sometimes | 18 | 3.5% | 11 | 2.5% | 9 | 2.1% | |
| n = 520 | n = 442 | n = 426 | |||||
| Ability to purchase cleaning product | Yes | 161 | 39.9% | 128 | 50.4% | 172 | 44.3% |
| No | 242 | 60.05% | 126 | 49.6 | 216 | 55.7% | |
| n = 403 | n = 254 | n = 388 | |||||
| Water Treatment Works | Type of Chlorine | Availability of the Chlorine | How Often Is Water Tested for Faecal Contaminants and Possible Pathogens? | Does the Plant Provide Enough Water to the Community? | If No, Why? |
|---|---|---|---|---|---|
| WTW1 | Calcium hypochlorite | Always available | Once a year | No | Pipeline blocked |
| WTW2 | Chlorine gas | Always available | Once a week | Yes | NA |
| WTW3 | Chlorine gas | Available for a period of 1 to 2 weeks | Everyday | Yes | NA |
| WTW4 | Calcium hypochlorite and chlorine gas | Always available | Everyday | Yes | NA |
| WTW5 | Calcium hypochlorite and chlorine gas | Always available | Once a month | No | High water demand |
| Wastewater Treatment Plants | Where Is the Wastewater Coming from? | Ability to Effectively Manage the Waste Received | Have You Ever Experienced Any Difficulties during Wastewater Treatment? | If Yes, How Did You Overcome That? | Is the Equipment up to Standard or Need Repair or Replacement? | What Is the Wastewater Used for after Treatment? |
|---|---|---|---|---|---|---|
| WWTW1 | Malls, townships, hospitals, and mortuaries | Able | Yes, during floods | Bypass to maturation ponds | Repairs needed | Supplies water to water sources (rivers) |
| WWTW2 | Malls, townships, hospitals, and mortuaries | Able | Yes, during floods | Nothing | Repairs needed | Supplies water to water sources (rivers) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murei, A.; Mogane, B.; Mothiba, D.P.; Mochware, O.T.W.; Sekgobela, J.M.; Mudau, M.; Musumuvhi, N.; Khabo-Mmekoa, C.M.; Moropeng, R.C.; Momba, M.N.B. Barriers to Water and Sanitation Safety Plans in Rural Areas of South Africa—A Case Study in the Vhembe District, Limpopo Province. Water 2022, 14, 1244. https://doi.org/10.3390/w14081244
Murei A, Mogane B, Mothiba DP, Mochware OTW, Sekgobela JM, Mudau M, Musumuvhi N, Khabo-Mmekoa CM, Moropeng RC, Momba MNB. Barriers to Water and Sanitation Safety Plans in Rural Areas of South Africa—A Case Study in the Vhembe District, Limpopo Province. Water. 2022; 14(8):1244. https://doi.org/10.3390/w14081244
Chicago/Turabian StyleMurei, Arinao, Barbara Mogane, Dikeledi Prudence Mothiba, Opelo Tlotlo Wryl Mochware, Jeridah Matlhokha Sekgobela, Mulalo Mudau, Ndamulelo Musumuvhi, Colette Mmapenya Khabo-Mmekoa, Resoketswe Charlotte Moropeng, and Maggie Ndombo Benkete Momba. 2022. "Barriers to Water and Sanitation Safety Plans in Rural Areas of South Africa—A Case Study in the Vhembe District, Limpopo Province" Water 14, no. 8: 1244. https://doi.org/10.3390/w14081244