
Practitioners’ Perspective on the Prevalent Water Quality Management Practices for Legionella Control in Large Buildings in the United States

 , and
, and
Abstract
:
1. Introduction
2. Methods
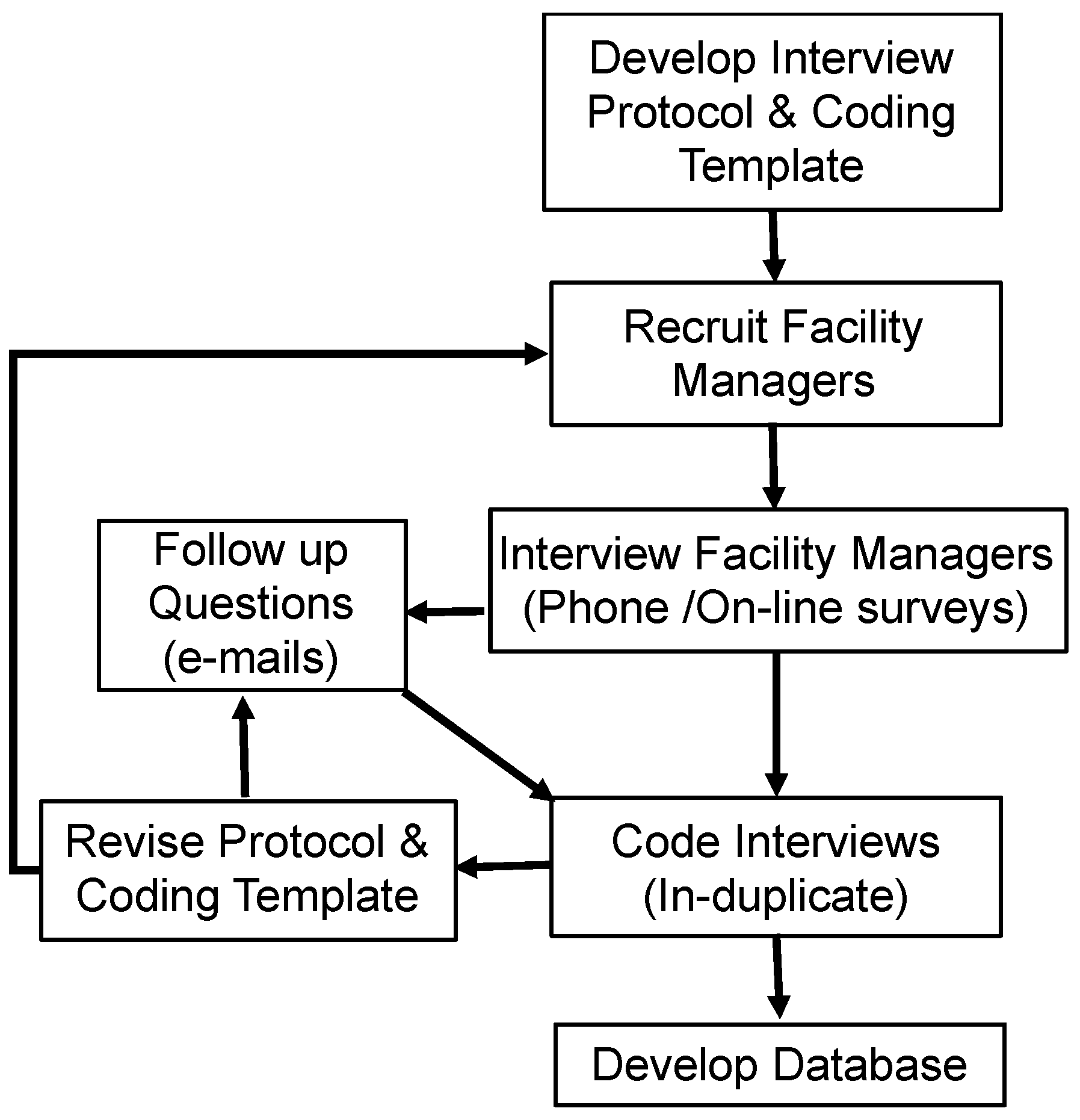
2.1. Interview Protocols
2.2. Recruitment of Building Water Quality Managers
2.3. Data Collection and Coding Responses
2.4. Database Processing
2.5. Statistical Analyses
3. Results
3.1. Database Characteristics
3.2. Water Quality Monitoring, Management Plans, and Control Measures
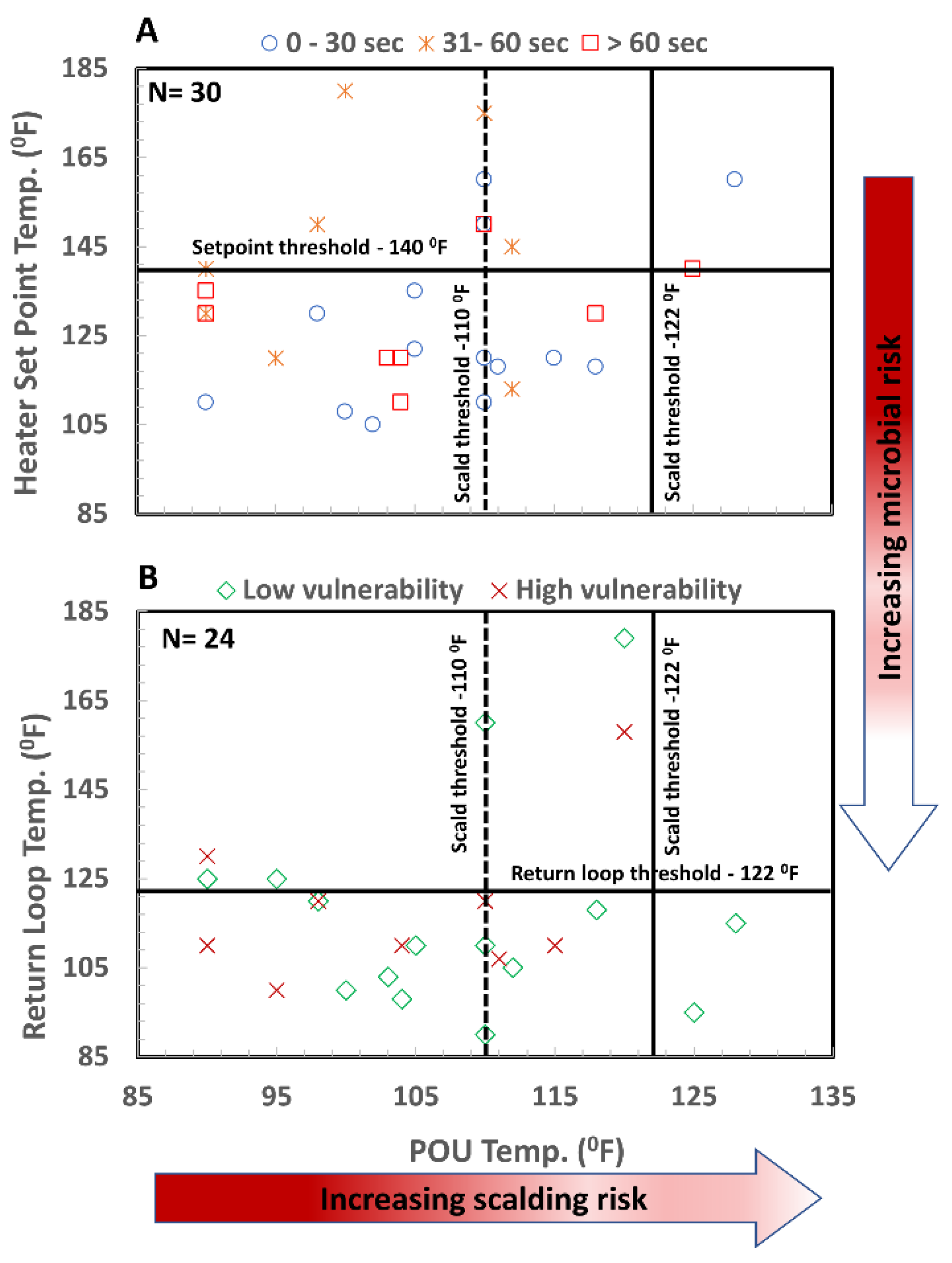
3.3. Temperature Monitoring
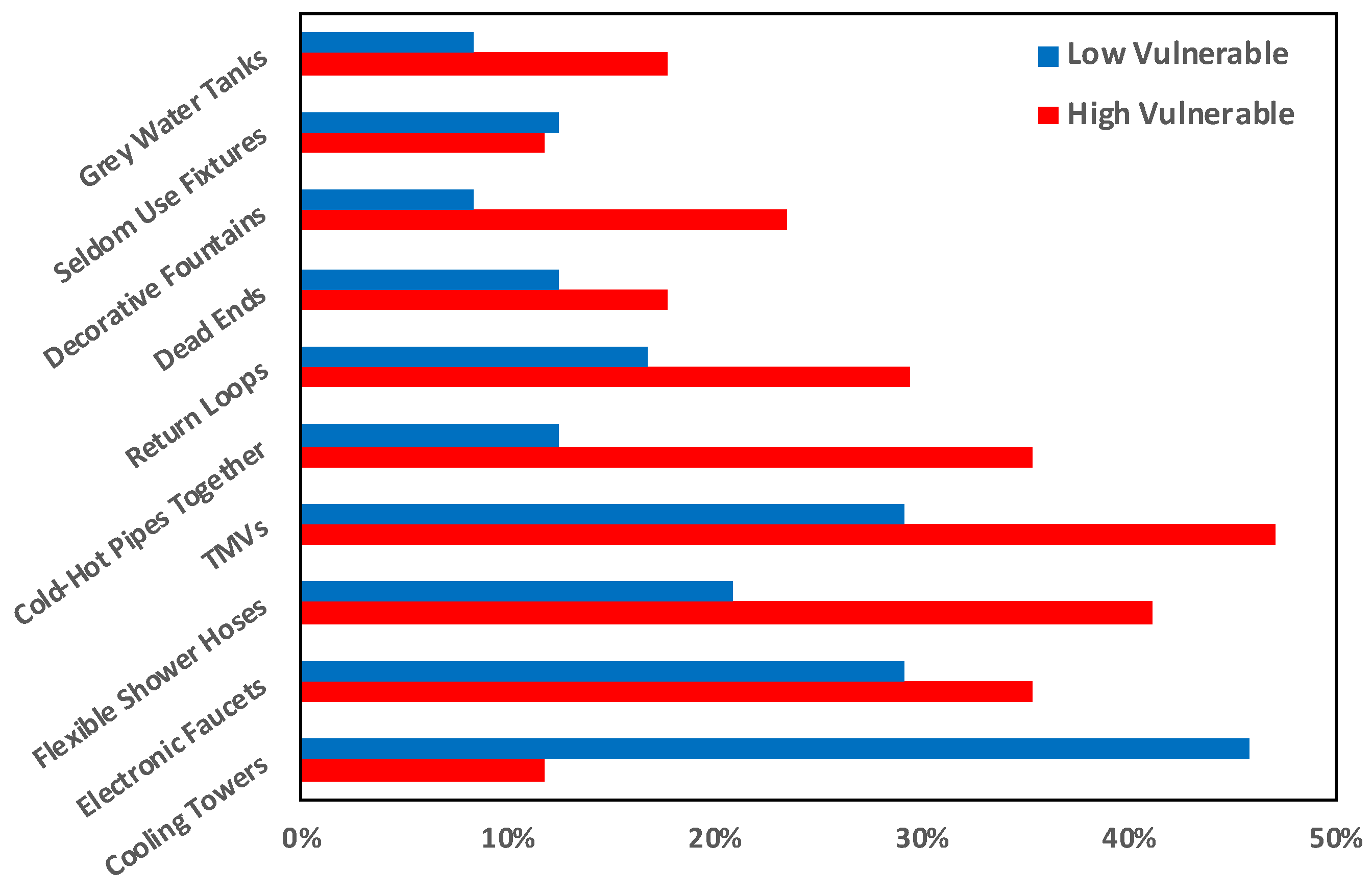
3.4. Potentially Problematic Features in Building Plumbing Systems
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bradley, T.C.; Haas, C.N.; Sales, C.M. Nitrification in Premise Plumbing: A Review. Water 2020, 12, 830. [Google Scholar] [CrossRef] [Green Version]
- Montagna, M.T.; De Giglio, O.; Napoli, C.; Diella, G.; Rutigliano, S.; Agodi, A.; Auxilia, F.; Baldovin, T.; Bisetto, F.; Arnoldo, L.; et al. Control and Prevention Measures for Legionellosis in Hospitals: A Cross-Sectional Survey in Italy. Environ. Res. 2018, 166, 55–60. [Google Scholar] [CrossRef]
- Haubitz, S.; Hitz, F.; Graedel, L.; Batschwaroff, M.; Wiemken, T.L.; Peyrani, P.; Ramirez, J.A.; Fux, C.A.; Mueller, B.; Schuetz, P. Ruling out Legionella in Community-Acquired Pneumonia. Am. J. Med. 2014, 127, 1010-e11. [Google Scholar] [CrossRef] [PubMed]
- Barskey, A.; Lackraj, D.; Tripathi, P.S.; Cooley, L.; Lee, S.; Smith, J.; Edens, C. Legionnaire’s Disease Surveillance Summary Report, United States 2016–2017; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2020; p. 50.
- Pauli, B.J. The Flint Water Crisis. WIREs Water 2020, 7, e1420. [Google Scholar] [CrossRef]
- Julien, R.; Dreelin, E.; Whelton, A.J.; Lee, J.; Aw, T.G.; Dean, K.; Mitchell, J. Knowledge Gaps and Risks Associated with Premise Plumbing Drinking Water Quality. AWWA Water Sci. 2020, 2, e1177. [Google Scholar] [CrossRef]
- Proctor, C.R.; Rhoads, W.J.; Keane, T.; Salehi, M.; Hamilton, K.; Pieper, K.J.; Cwiertny, D.M.; Prévost, M.; Whelton, A.J. Considerations for Large Building Water Quality after Extended Stagnation. AWWA Water Sci. 2020, 2, e1186. [Google Scholar] [CrossRef] [PubMed]
- Van Kenhove, E.; Dinne, K.; Janssens, A.; Laverge, J. Overview and Comparison of Legionella Regulations Worldwide. Am. J. Infect. Control 2019, 47, 968–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, R.; Hamilton, K.A.; Rasheduzzaman, M.; Yang, Z.; Kar, S.; Fasnacht, A.; Masters, S.V.; Gurian, P.L. Managing Water Quality in Premise Plumbing: Subject Matter Experts’ Perspectives and a Systematic Review of Guidance Documents. Water 2020, 12, 347. [Google Scholar] [CrossRef] [Green Version]
- Bédard, E.; Fey, S.; Charron, D.; Lalancette, C.; Cantin, P.; Dolcé, P.; Laferrière, C.; Déziel, E.; Prévost, M. Temperature Diagnostic to Identify High Risk Areas and Optimize Legionella pneumophila Surveillance in Hot Water Distribution Systems. Water Res. 2015, 71, 244–256. [Google Scholar] [CrossRef]
- U.S. EPA. Drinking Water Criteria Document For Legionella (Final Draft); Environmental Criteria and Assessment Office: Washington, DC, USA, 1985.
- OSHA. Legionnaires’ Disease: Section II: What Water Systems in Workplaces Are Potential Sources of Legionnaires’ Bacteria (LDB)? OSHA: Washington, DC, USA, 1996.
- CDC. Annex to the Model Aquatic Health Code: Scientific Rationale; Centers for Disease Control: Atlanta, GA, USA, 2016. Available online: https://www.cdc.gov/mahc/pdf/2016-mahc-annex-final.pdf (accessed on 7 February 2022).
- CDC. What Clinicians Need to Know about Legionnaires’ Disease; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2017.
- Department of Veterans Affairs VHA. Directive 2008-010 Prevention of Legionella Disease; Department of Veterans Affairs: Washington, DC, USA, 2008.
- Department of Veterans Affairs VHA. Directive 1061: Prevention of Healthcare-Associated Legionella Disease and Scald Injury from Potable Water Distribution Systems; Department of Veterans Affairs: Washington, DC, USA, 2014.
- ASHRAE. ANSI/ASHRAE Standard 188-2018 Legionellosis: Risk Management for Building Water Systems; American Society of Heating, Refrigerating and Air-Conditioning Engineers: Peachtree Corners, GA, USA, 2018; p. 24. [Google Scholar]
- NASEM. Management of Legionella in Water Systems; The National Academies Press: Washington, DC, USA, 2019. [Google Scholar]
- Bartram, J.; Chartier, Y.; Lee, J.V.; Pond, K.; Surman-Lee, S. Legionella and the Prevention of Legionellosis; World Health Organization (WHO): Geneva, Switzerland, 2007; ISBN 92-4-156297-8. [Google Scholar]
- WHO. Water Safety in Buildings. Paper Presented at the World Health Organization (WHO), Geneva, Switzerland. Available online: http://apps.who.int/iris/bitstream/10665/76145/1/9789241548106_eng.pdf (accessed on 29 November 2017).
- Government of Western Australia, Department of Commerce, Department of Mines and Petroleum. Code of Practice Prevention and Control of Legionnaires’ Disease; Perth, Australia, 2010. Available online: https://www.commerce.wa.gov.au/sites/default/files/atoms/files/legionnaires-code.pdf (accessed on 7 February 2022).
- European Guidelines Working Group. European Technical Guidelines for the Prevention, Control and Investigation, of Infections Caused by Legionella Species; European Society of Clinical Microbiology and Infectious Disease: Basel, Switzerland, 2017. [Google Scholar]
- NYC. Health Cooling Tower Requirements: What Building Owners Should Know; New York City Department of Health and Mental Hygiene: New York, NY, USA, 2016.
- NYC. Heath Notice of Adoption of Chapter 8 (Cooling Towers) of Title 24 of the Rules of the City of New York; New York City Department of Health and Mental Hygiene: New York, NY, USA, 2016.
- Centers for Medicare & Medicaid Services (CMS). Memorandum to State Survey Agency Directors; Center for Medicare and Medicaid Service: Washington, DC, USA, 2017.
- ASHRAE. BSR/ASHRAE Standard 188P: Prevention of Legionellosis Associated With Building Water Systems (Second Public Review Draft); American Society of Heating, Refrigeration, and Air Conditioning Engineers: Atlanta, GA, USA, 2011. [Google Scholar]
- Codony, F.; Alvarez, J.; Oliva, J.M.; Ciurana, B.; Company, M.; Camps, N.; Torres, J.; Minguell, S.; Jové, N.; Cirera, E.; et al. Factors Promoting Colonization by Legionellae in Residential Water Distribution Systems: An Environmental Case-Control Survey. Eur. J. Clin. Microbiol. Infect. Dis. 2002, 21, 717–721. [Google Scholar] [CrossRef]
- O’Loughlin, R.E.; Kightlinger, L.; Werpy, M.C.; Brown, E.; Stevens, V.; Hepper, C.; Keane, T.; Benson, R.F.; Fields, B.S.; Moore, M.R. Restaurant Outbreak of Legionnaires’ Disease Associated with a Decorative Fountain: An Environmental and Case-Control Study. BMC Infect. Dis. 2007, 7, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Edwards, M.; Falkinham, J.O.; Pruden, A. Molecular Survey of the Occurrence of Legionella spp., Mycobacterium spp., Pseudomonas aeruginosa, and Amoeba Hosts in Two Chloraminated Drinking Water Distribution Systems. Appl. Environ. Microbiol. 2012, 78, 6285–6294. [Google Scholar] [CrossRef] [Green Version]
- Kuroki, T.; Watanabe, Y.; Teranishi, H.; Izumiyama, S.; Amemura-Maekawa, J.; Kura, F. Legionella Prevalence and Risk of Legionellosis in Japanese Households. Epidemiol. Infect. 2017, 145, 1398–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, J.; Struewing, I.; Vereen, E.; Kirby, A.E.; Levy, K.; Moe, C.; Ashbolt, N. Molecular Detection of Legionella spp. and Their Associations with Mycobacterium spp., Pseudomonas aeruginosa and Amoeba Hosts in a Drinking Water Distribution System. J. Appl. Microbiol. 2016, 120, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Suarez, A.; Araujo, R. Evaluation of Legionella Presence in the Water System of a Public Building by Semi-Nested Polymerase Chain Reaction as a Rapid Screening Method Complementary to Plate Count. Water Sci. Technol.-Water Supply 2013, 13, 1560–1568. [Google Scholar] [CrossRef]
- Bargellini, A.; Marchesi, I.; Righi, E.; Ferrari, A.; Cencetti, S.; Borella, P.; Rovesti, S. Parameters Predictive of Legionella Contamination in Hot Water Systems: Association with Trace Elements and Heterotrophic Plate Counts. Water Res. 2011, 45, 2315–2321. [Google Scholar] [CrossRef] [PubMed]
- Arvand, M.; Jungkind, K.; Hack, A. Contamination of the Cold Water Distribution System of Health Care Facilities by Legionella Pneumophila: Do We Know the True Dimension? Eurosurveillance 2011, 16, 19844. [Google Scholar] [CrossRef]
- Martinelli, F.; Caruso, A.; Moschini, L.; Turano, A.; Scarcella, C.; Speziani, F. A Comparison of Legionella Pneumophila Occurrence in Hot Water Tanks and Instantaneous Devices in Domestic, Nosocomial, and Community Environments. Curr. Microbiol. 2000, 41, 374–376. [Google Scholar] [CrossRef]
- Stout, J.E.; Muder, R.R.; Mietzner, S.; Wagener, M.M.; Perri, M.B.; DeRoos, K.; Goodrich, D.; Arnold, W.; Williamson, T.; Ruark, O.; et al. Role of Environmental Surveillance in Determining the Risk of Hospital-Acquired Legionellosis: A National Surveillance Study with Clinical Correlations. Infect. Control Hosp. Epidemiol. 2007, 28, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Stout, J.; Yu, V.L.; Vickers, R.M.; Zuravleff, J.; Best, M.; Brown, A.; Yee, R.B.; Wadowsky, R. Ubiquitousness of Legionella Pneumophila in the Water Supply of a Hospital with Endemic Legionnaires’ Disease. N. Engl. J. Med. 1982, 306, 466–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CDC. Guidelines for Environmental Infection Control in Health-Care Facilities: Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC); CDC: Atlanta, GA, USA, 2003.
- HSE. Programme of Interventions for Controlling Legionella Risks in Workplaces 2013–14: Half-Year Report; Health and Safety Executive: London, UK, 2013.
- DH Estates and Facilities Division. HTM 04-01 The Control of Legionella, Hygiene, “Safe” Hot Water, Cold Water and Drinking Water Systems. Part B: Operational Management; National Health Service: London, UK, 2006.
- Whiley, H. Legionella Risk Management and Control in Potable Water Systems: Argument for the Abolishment of Routine Testing. Int. J. Environ. Res. Public Health 2017, 14, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasheduzzaman, M.; Singh, R.; Haas, C.N.; Gurian, P.L. Required Water Temperature in Hotel Plumbing to Control Legionella Growth. Water Res. 2020, 182, 115943. [Google Scholar] [CrossRef]
- International Code Council. 2015 International Plumbing Code; The International Code Council: Washington, DC, USA, 2015. [Google Scholar]
- ASPE. Domestic Hot Water Systems: Continuing Education from the American Society of Plumbing Engineers; American Society of Plumbing Engineers: Rosemont, IL, USA, 2015. [Google Scholar]
- Niedeveld, C.J.; Pet, F.M.; Meenhorst, P.L. Effect of Rubbers and Their Constituents on Proliferation of Legionella Pneumophila in Naturally Contaminated Hot Water. Lancet 1986, 2, 180–184. [Google Scholar] [CrossRef]
- van der Lugt, W.; Euser, S.M.; Bruin, J.P.; Den Boer, J.W.; Walker, J.T.; Crespi, S. Growth of Legionella Anisa in a Model Drinking Water System to Evaluate Different Shower Outlets and the Impact of Cast Iron Rust. Int. J. Hyg. Environ. Health 2017, 220, 1295–1308. [Google Scholar] [CrossRef] [PubMed]
- Department of Health (DH). Health Technical Memorandum 04-01 Addendum: Pseudomonas aeruginosa–Advice for Augmented Care Units; Department of Health: London, UK, 2013.
- Sydnor, E.R.M.; Bova, G.; Gimburg, A.; Cosgrove, S.E.; Perl, T.M.; Maragakis, L.L. Electronic-Eye Faucets: Legionella Species Contamination in Healthcare Settings. Infect. Control Hosp. Epidemiol. 2012, 33, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Cullom, A.C.; Martin, R.L.; Song, Y.; Williams, K.; Williams, A.; Pruden, A.; Edwards, M.A. Critical Review: Propensity of Premise Plumbing Pipe Materials to Enhance or Diminish Growth of Legionella and Other Opportunistic Pathogens. Pathogens 2020, 9, 957. [Google Scholar] [CrossRef] [PubMed]
- Falkinham, J.O. Living with Legionella and Other Waterborne Pathogens. Microorganisms 2020, 8, 2026. [Google Scholar] [CrossRef]
- Hamilton, K.A.; Prussin, A.J.; Ahmed, W.; Haas, C.N. Outbreaks of Legionnaires’ Disease and Pontiac Fever 2006–2017. Curr. Environ. Health Rep. 2018, 5, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Rasheduzzaman, M. Managing Water Quality in Premise Plumbing: Application of Systematic Review, Meta-Analysis and the Delphi Method for Decision Making. Ph.D. Thesis, Drexel University, Philadelphia, PA, USA, 2021. [Google Scholar]
- Galada, H.C.; Gurian, P.L.; Olson, M.S.; Teng, J.; Kumar, A.; Wardell, M.; Eggers, S.; Casman, E. Development of Failure Scenarios for Biosolids Land Application Risk Assessment. Water Environ. Res. 2013, 85, 141–150. [Google Scholar] [CrossRef]
- Galada, H.C.; Gurian, P.L.; Hong, T. First Responder Knowledge and Training Needs for Bioterrorism. J. Homel. Secur. Emerg. Manag. 2013, 10, 631–660. [Google Scholar] [CrossRef]
- Abualfaraj, N.; Gurian, P.L.; Olson, M.S. Frequency Analysis of Failure Scenarios from Shale Gas Development. Int. J. Environ. Res. Public Health 2018, 15, 885. [Google Scholar] [CrossRef] [Green Version]
- Awada, M.; Becerik-Gerber, B.; White, E.; Hoque, S.; O’Neill, Z.; Pedrielli, G.; Wen, J.; Wu, T. Occupant Health in Buildings: Impact of the COVID-19 Pandemic on the Opinions of Building Professionals and Implications on Research. Build. Environ. 2022, 207, 108440. [Google Scholar] [CrossRef] [PubMed]
- ASPE. Plumbing Components and Equipment. In Plumbing Engineering Design Handbook—A Plumbing Engineer’s Guide to System Design and Specifications; American Society of Plumbing Engineers: Chicago, IL, USA, 2008; Volume 4. [Google Scholar]
- ASPE. Domestic Water Heating Design Manual, 2nd ed.; American Society of Plumbing Engineers: Rosemont, IL, USA, 2003. [Google Scholar]
- Tolofari, D.; Bartrand, T.; Masters, S.V.; Batista, M.D.; Haas, C.N.; Olson, M.S.; Gurian, P.L. Influence of Hot Water Temperature and Use Patterns on Microbial Water Quality in Building Plumbing System. Environ. Eng. Sci. 2021, 1–11. [Google Scholar] [CrossRef]
- Donohue, M.J.; O’Connell, K.; Vesper, S.J.; Mistry, J.H.; King, D.; Kostich, M.; Pfaller, S. Widespread Molecular Detection of Legionella Pneumophila Serogroup 1 in Cold Water Taps across the United States. Environ. Sci. Technol. 2014, 48, 3145–3152. [Google Scholar] [CrossRef]
- Hicks, L.A.; Garrison, L.E.; Nelson, G.E. Legionellosis--United States, 2000–2009. MMWR Morb. Mortal. Wkly. Rep. 2011, 60, 1083–1086. [Google Scholar]
- CDC. Legionella (Legionnaires’ Disease and Pontiac Fever). Available online: https://www.cdc.gov/Legionella/about/causes-transmission.html (accessed on 16 August 2017).
- CDC. Legionnaires’ Disease Surveillance Summary Report, 2014–2015; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2018.
- CDC. Surveillance and Reporting Resources. Available online: https://www.cdc.gov/legionella/health-depts/surv-reporting/case-definitions.html (accessed on 29 August 2021).
- Amoueyan, E.; Ahmad, S.; Eisenberg, J.N.S.; Pecson, B.; Gerrity, D. Quantifying Pathogen Risks Associated with Potable Reuse: A Risk Assessment Case Study for Cryptosporidium. Water Res. 2017, 119, 252–266. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, K.A.; Ahmed, W.; Toze, S.; Haas, C.N. Human Health Risks for Legionella and Mycobacterium avium Complex (MAC) from Potable and Non-Potable Uses of Roof-Harvested Rainwater. Water Res. 2017, 119, 288–303. [Google Scholar] [CrossRef]
- Hamilton, K.A.; Ahmed, W.; Palmer, A.; Smith, K.; Toze, S.; Haas, C.N. Seasonal Assessment of Opportunistic Premise Plumbing Pathogens in Roof-Harvested Rainwater Tanks. Environ. Sci. Technol. 2017, 51, 1742–1753. [Google Scholar] [CrossRef]
- Hamilton, K.A.; Hamilton, M.T.; Johnson, W.; Jjemba, P.; Bukhari, Z.; LeChevallier, M.; Haas, C.N.; Gurian, P.L. Risk-Based Critical Concentrations of Legionella Pneumophila for Indoor Residential Water Uses. Environ. Sci. Technol. 2019, 53, 4528–4541. [Google Scholar] [CrossRef] [Green Version]
- Rasheduzzaman, M.; Singh, R.; Haas, C.N.; Tolofari, D.; Yassaghi, H.; Hamilton, K.A.; Yang, Z.; Gurian, P.L. Reverse QMRA as a Decision Support Tool: Setting Acceptable Concentration Limits for Pseudomonas Aeruginosa and Naegleria Fowleri. Water 2019, 11, 1850. [Google Scholar] [CrossRef] [Green Version]
- Dean, K.; Mitchell, J. Reverse QMRA for Pseudomonas Aeruginosa in Premise Plumbing to Inform Risk Management. J. Environ. Eng. 2020, 146, 04019120. [Google Scholar] [CrossRef]
- Hozalski, R.M.; LaPara, T.M.; Zhao, X.; Kim, T.; Waak, M.B.; Burch, T.; McCarty, M. Flushing of Stagnant Premise Water Systems after the COVID-19 Shutdown Can Reduce Infection Risk by Legionella and Mycobacterium spp. Environ. Sci. Technol. 2020, 54, 15914–15924. [Google Scholar] [CrossRef] [PubMed]
- van Hoof, J.; Hornstra, L.M.; van der Blom, E.; Nuijten, O.W.; van der Wielen, P.W. The Presence and Growth of Legionella Species in Thermostatic Shower Mixer Taps: An Exploratory Field Study. Build. Serv. Eng. Res. Technol. 2014, 35, 600–612. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Developing a Water Management Program to Reduce Legionella Growth & Spread in Buildings: A Practical Guide to Implementing Industry Standards; US Department of Health and Human Services: Atlanta, GA, USA, 2017.
- ANSI/ASHRAE. ANSI/ASHRAE Standard 188-2015 Legionellosis: Risk Management for Building Water Systems; American Society of Heating Refrigeration and Air Conditioning Engineers: Peachtree Corners, GA, USA, 2015. [Google Scholar]
- Tolofari, D.L.; Masters, S.V.; Bartrand, T.; Hamilton, K.A.; Haas, C.N.; Olson, M.; Summers, R.S.; Rasheduzzaman, M.; Young, A.; Singh, R.; et al. Full factorial study of pipe characteristics, stagnation times, and water quality. AWWA Water Sci. 2020, 2, e1204. [Google Scholar] [CrossRef]
- Rhoads, W.J.; Prévost, M.; Pieper, K.J.; Keane, T.; Whelton, A.J.; Rölli, F.; Proctor, C.R.; Grimard-Conea, M. Responding to Water Stagnation in Buildings with Reduced or No Water Use: A Framework for Facility Managers; American Water Works Association: Denver, CO, USA, 2020. [Google Scholar]
- CDC. Reopening Buildings after Prolonged Shutdown or Reduced Operation. 2021. Available online: https://www.cdc.gov/nceh/ehs/water/legionella/building-water-system.html (accessed on 8 November 2021).
- Rasheduzzaman, M.; Singh, R.; Annapoorna Madireddy, L.; Gurian, P.L. Conceptualization to Development of a Decision Support Tool to Manage Building Water Quality. World Environ. Water Resour. Congr. U. S. 2021, 925–936. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Areas of Concern for Plumbing WQ | Topics Covered |
|---|---|
| Building characteristics | Building types (hospital, retirement homes/assisted living facilities, high rise apartments, hotels, academic institutions, commercial buildings, others); Greater or less than 10 stories; Centralized hot water system present or absent; Heater types (gas, electric, steam, others); Return loop present or absent |
| Monitoring parameters | Temperature at heater, faucet, return loop, distal tap; Time to tap; Hardness; pH; Microbes; Disinfectant residual; Others * |
| Problematic features | Dead ends; Cold and hot water pipes running together; TMVs; Grey water tanks; Cooling towers; Centralized atomizers/misters; Seldom used areas; Decorative fountains; Other water features; Hot tubs (spas); Flexible shower hoses; Electronic faucets; Return loop system; Heat recovery systems *; Solar water heater *; Manifold system *; Splashing faucets *; Laminar flow devices *; Other * |
| Control measures | Return loop monitor/flush/treat; Water treatment at sink or shower (softening, antimicrobial—UV, chlorine, chlorine dioxide, copper/silver); Shower head replaced/disinfected; Hoses drain to empty between usages; Flushing performed in laminar flow devices * |
| Management plans | Written plan for monitoring? Results archived? Challenges in managing monitoring record? * Support needed in managing records * |
| Guidance source | Guidance from CDC, ASHRAE, EPA, State, City, Utility, IPC, others (LEED, USGBC); Is additional information source required? * Type of information? * |
| Demographic information | Background—operation, design, or both; Years of experience |
| Factors | Shapiro–Wilk Normality Test | Mann–Whitney U Test/t-Test * | |||||
|---|---|---|---|---|---|---|---|
| Phone | Online Survey | W/t * | sig. (Two-Tailed, α = 0.05) | Difference in Median/Mean * (in °F/°C) | |||
| W Stats | sig. (α = 0.05) | W-Stats | sig. (α = 0.05) | ||||
| Setpoint Temp | 0.910 | 0.138 | 0.899 | 0.0389 | 141 | 0.776 | 0.0 |
| POU Temp * | 0.947 | 0.550 | 0.918 | 0.0612 | 243 | 2.00 × 10−3 | 11.3/6 |
| Recirculation Loop Temp | 0.956 | 0.782 | 0.889 | 0.0447 | 44.0 | 0.338 | −10.0/−6 |
| Time to Tap | 0.720 | 8.89 × 10−4 | 0.772 | 1.06 × 10−4 | 152 | 0.890 | −1.0/−1 |
| Monitoring Parameters | Management Plan | Control Measures | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameters | Low vuln. | High vuln. | Parameters | Low vuln. | High vuln. | Parameters | Low vuln. | High vuln. | |
| Temp. at heater setpoint | 88% | 82% | Written plan | 29% | 59% | Return loop monitoring/flush/treat | 54% | 59% | |
| Temp. at faucet/POU | 88% | 94% | Results archived | 21% | 47% | ||||
| Temp. at return loop | 67% | 59% | Information source | CDC | 4% | 18% | Water treatment at sink/shower | 33% | 59% |
| Temp. at distal tap | 21% | 35% | ASHRAE | 25% | 6% | ||||
| Time to Tap | 92% | 88% | EPA guidance | 4% | 18% | Shower head replaced/disinfected | 25% | 29% | |
| Hardness | 25% | 24% | State guidance | 13% | 29% | ||||
| pH | 25% | 24% | City guidance | 21% | 12% | Self-draining showers | 33% | 65% | |
| Microbes | 38% | 41% | Utility guideline | 0% | 6% | ||||
| Residual disinfectant | 4% | 6% | IPC | 21% | 12% | ||||
| Others | 13% | 12% | None | 8% | 0% | ||||
| Parameters | Interview Response °F (°C) | Buildings in Compliance Total (Low Vuln., High Vuln.) | Guidance for Microbial Control (Except as Noted) °F (°C) or Seconds. | References | |
|---|---|---|---|---|---|
| Water Heater Set Point Temp | N = 35 | 37% (33%, 43%) | ≥140 (≥60) | OSHA, 1996 [12] CDC, 2003 [38] WHO, 2007 [20] EGWG, 2017 [22] NASEM, 2020 [18] | |
| Median = 130 (54) | |||||
| Range = 105–192 (41–89) | |||||
| St. Dev. = 21 (12) | |||||
| Point-of-Use or Faucet Temperature | N = 36 | 47% (52%, 40%) | <110 (<43) (To control scald risk) | WHO, 2011 IPC, 2015 [43] | |
| Median = 110 (43) | |||||
| Range = 90–128 (32–53) | 94% (90%, 100%) | <122–124 (<50–51) To control scald risk | DVA, 2014 [16] EGWG, 2017 [22] | ||
| St. Dev. = 11 (6) | |||||
| Recirculation Loop Temperature | N = 24 | 25% (27%, 22%) | ≥122 (≥50) | WHO 2007 [19] EGWG 2017 [22] | |
| Median = 110 (43) | |||||
| Range = 90–179 (32–82) | |||||
| St. Dev. = 20 (11) | |||||
| Temperature Loss in Plumbing (Set Point—Recirculation Loop) | N = 22 | 26% (39%, 15%) | <9 (<5) | ASPE, 2008 [57] | |
| Median = 13 (7) | |||||
| St. Dev. = 12 (7) | |||||
| Hot Water Temperature Time to Tap | 0–30 s 31–60 s >60 s | (N = 18; 49%) (N = 9; 24%) (N = 10; 27%) | 73% (73%, 73%) | 122–131 °F (50–55 °C) at POU in 60 Sec | EGWG, 2017 [22] |
| ≥131 °F (≥55 °C) at distal point in 60 Sec | NASEM, 2020 [18] | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singh, R.; Chauhan, D.; Fogarty, A.; Rasheduzzaman, M.; Gurian, P.L. Practitioners’ Perspective on the Prevalent Water Quality Management Practices for Legionella Control in Large Buildings in the United States. Water 2022, 14, 663. https://doi.org/10.3390/w14040663
Singh R, Chauhan D, Fogarty A, Rasheduzzaman M, Gurian PL. Practitioners’ Perspective on the Prevalent Water Quality Management Practices for Legionella Control in Large Buildings in the United States. Water. 2022; 14(4):663. https://doi.org/10.3390/w14040663
Chicago/Turabian StyleSingh, Rajveer, Deepika Chauhan, Alanna Fogarty, Md Rasheduzzaman, and Patrick L. Gurian. 2022. "Practitioners’ Perspective on the Prevalent Water Quality Management Practices for Legionella Control in Large Buildings in the United States" Water 14, no. 4: 663. https://doi.org/10.3390/w14040663