
Risk Analysis of Otitis Externa (Swimmer’s Ear) in Children Pool Swimmers: A Case Study from Greece



Department of Public Health, Medical School, University of Patras, 26504 Patras, Greece
*
Author to whom correspondence should be addressed.
Water 2022, 14(13), 1983; https://doi.org/10.3390/w14131983
Submission received: 30 April 2022
/
Revised: 3 June 2022
/
Accepted: 16 June 2022
/
Published: 21 June 2022
(This article belongs to the Special Issue Healthy Recreational Waters: Sanitation and Safety Issues)
Abstract
:Otitis is an ear inflammation characterized by an accumulation of polluted fluids in the ear, inflating the drum, causing ear pain, and draining the mucous membrane (pus) into the ear canal if the drum is perforated. Swimmer’s otitis, also known as acute external otitis, is a medical condition that frequently affects competitive swimmers. The risk factor analysis study was based on data obtained between May 2018 and May 2019 from four public swimming pools in Patras, Achaia. A checklist was created to evaluate the pools’ operational conditions, and it included information on the pools’ sanitation as well as swimming pool hygiene guidelines. In addition, a questionnaire was devised to collect data on pool swimmers’ use of the pools. Microbiological testing of the pool water was done ahead of time, and data on external otitis cases from hospitals was gathered. Based on this information, a risk factor analysis was conducted. Gender, weight, and age do not appear to have an impact on the number of otitis media cases that occur because of swimming in the pools. There is also no statistically significant link between episodes and the frequency of otitis events in locker rooms, restrooms, or swimming pools. The frequency with which swimmers utilize the pool, rather than the pool’s microbial burden, is the most significant determinant in otitis episodes. Furthermore, there is no statistically significant link between chlorine odor and otitis episodes. Additionally, several abnormalities in the ear or the child’s history do not appear to affect otitis episodes. More research is needed to determine whether infections are linked to microbial load or if other factors are responsible for the emergence of waterborne infections.
1. Introduction
Otitis is the inflammation of the ear described by an accumulation of contaminated liquid in the ear, inflating the drum, provoking ear pain, and, if the drum is pierced, draining the mucous membrane (pus) into the ear canal [1]. Swimmer’s otitis or acute external otitis is a pathological situation that often occurs in those who swim competitively [2].
The conservation of swimmers’ health is of prime importance while using swimming pools. The absence of antiseptic chemical compounds in the water, in the appropriate quantity, could lead to infectious diseases [3]. There are plenty of infectious diseases that can be transmitted by recreational water. These diseases include skin, ear, and eye infections, and gastroenteritis [4]. There are many microbiological pathogens that could cause waterborne diseases such as parasites, bacteria, and viruses [5,6]. Pseudomonas aeruginosa infects swimmers’ ears (pools) and Staphylococcus aureus infects the skin, wounds, and ears and the sources are from bathers shedding in pool water [7]. Waterborne diseases have momentous repercussions both locally and globally [8]. As a result, it is necessary to reduce the levels of microorganisms in recreational waters to combat the health hazards related to swimming [4].
Pool-related Pseudomonas aeruginosa infections principally provoke folliculitis and external otitis. P. aeruginosa creates biofilms on surfaces in the pool environment [9]. These bacteria persist and reproduce under low nutrient conditions. The temperature conditions range from 5 to 42 °C, and the pool’s warm and humid conditions are suitable for its growth [10]. As a result, a correlation between the development of otitis and swimming in water contaminated with the bacteria P. aeruginosa has been recorded [11,12]. There is also proof that otitis is directly connected with the presence of moisture [13]. There are factors that boost the rapid growth of P. aeruginosa. Such factors include long periods of exposure to moisture with an increased risk of cerumen loss, and increased water temperatures [14,15]. As a result, these factors distribute an explicit causal mechanism for the remarkable connection between the incidence of P. aeruginosa and humidity.
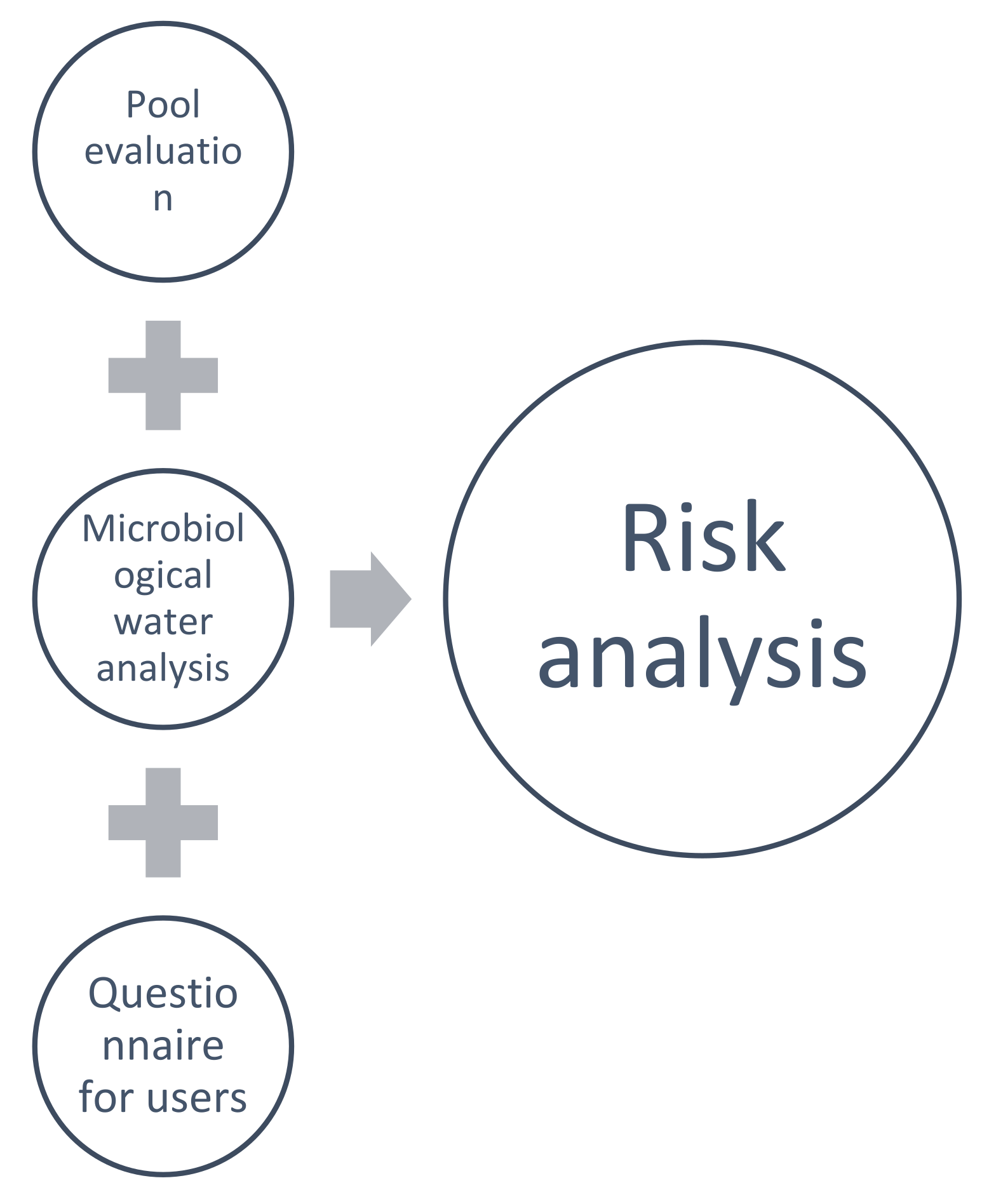
This study aimed to analyze and evaluate potential risk factors of otitis externa in children pool swimmers. The risk analysis study was conducted based on data from the four public swimming pools in Patras, Achaia. A checklist has been developed to evaluate the working conditions of the pools including information on the sanitation of swimming pool facilities as well as the hygiene rules regarding swimming pool use. Additionally, a questionnaire was created for the use of the swimming pool by the pool swimmers. In advance, microbiological analysis of the pool water was performed and data for external otitis cases from hospitals were collected. Risk analysis was performed based on this data.
2. Methods
2.1. Study Design
The study was conducted at the four public swimming pools in Patras, Achaia between May 2018 and May 2019. A checklist was developed to evaluate the working conditions of the pools. The checklist included information on the sanitation of the swimming pool facilities as well as the hygiene rules regarding swimming pool use.
Additionally, a questionnaire was created for the use of the swimming pools by the pool swimmers. The final structure of the questionnaire consisted of the following sections:
Demographics with 13 questions: (1) gender, (2) age, (3) height, (4) body weight, (5) place of residence, (6) citizenship, (7) swimming pool, (8) father’s age, (9) mother’s age, (10) family income, (11, 12) parents’ educational level, (13) frequency of use of a swimming pool in the given period (Figure 1).
Personal history of the child and episodes of otitis with 6 questions: (14) diseases during the study period May 2018–May 2019, (15) existence of diagnosed ear abnormality, (17) otitis episodes in the interval between May 2018–May 2019, (18) number of otitis episodes, (19) total otitis episodes in that period.
Treatment, recovery, and effects on daily activities with 8 questions: (20) treatment for otitis externa, (21) what treatment, (22) if use of the pool was discontinued, (23) consulted physician, (24) public or private physician, (25) response to treatment, (26) recovery time, (27) abstinence from normal obligations.
Child’s health and preventive exams: (35) what was the child’s health status in the last year, (36) had he/she encountered a health problem, (37) what kind of help is obtained when the child has a health problem, (38) how many days did you wait until you went to the doctor?
2.2. Water Sampling
Pool water samples were collected from the middle of the swimming pool at a depth of 25 cm [16]. At the time of collection, pH, residual chlorine, and temperature of the samples were recorded [17]. Samples of 1000 mL were collected in sterile plastic bottles within 30 s of the establishment of backwash ejection. Sampling bottles contained sodium thiosulfate (0.025% w/v) to neutralize any residual chlorine present. Then, they were stored at 4 °C and transported directly to the laboratory where they were analyzed within 24 h of receipt [18,19]. The periodicity of sample collection was once a week on random days and hours, according to World Health Organization (WHO) [7].
2.3. Microbiological Analysis of Pool Water
When the samples arrived in the laboratory, the conductivity of the pool water was recorded [20]. Standard cultural methods were used for the detection of the total coliform count, E. coli, total viable count, Pseudomonas aeruginosa, and Staphylococcus aureus [17]. Pseudomonas aeruginosa infects swimmers’ ears (pools) and Staphylococcus aureus infects skin, wounds, and ears and the source is bathers’ shedding in pool water [7]. Fecal coliforms/E. coli were analyzed according to ISO 9308-1, Total viable count was according to Yedeme et al. [17], while Pseudomonas aeruginosa was analyzed according to ISO 16,266 and Staphylococcus aureus according to the National Public Health Service guidelines.
2.4. Statistics
Statistical analysis of the differences among age groups and between the male and female swimmers was performed via IBM SPSS v25 (SPSS, NC). Given that we did not have a firmly preconceived notion of what the relationship between swimming and otitis episodes should be or where the cut-points might fall, an ANOVA analysis was used to determine the reasonable cut-point values of pool use should be, and where age/gender might lie based on the greatest reduction within the group standard deviation. For illustrative purposes, descriptive analysis of distributions of swimming was developed by excel separately for children’s groups and different pools.
3. Results
3.1. Sampling
The four swimming pools that were included in the sample participated with the following rates of sampling and questionnaires:
- SP1 37.39%.
- SP2 32.17%.
- SP3 22.6%.
- SP4 7.8%.
3.2. Microbiological Results
The water samples were collected from four swimming pools in the Patras area. The following data are an average of the weekly measurements taken from samples of the water from the swimming pools mentioned above (Table 1).
3.3. Questionnaires
The number of questionnaires was 230. The majority of the respondents were women, and the children were approximately divided, with boys accounting for 57.83% of the sample and girls 42.17%. The sample age of children was 23% younger than 5 years, 61.7% was 6–12 years, and 15.2% was 12–15 years. The height of the children in centimeters was divided and the categories that reached the highest percentages were 112 cm and 120 cm. Half of the sample were from 83 cm to 120 cm and the remaining 50% were from 121 to 188 cm. In 50% of the samples, the weight of children was from 12 to 27 kg and the remaining 50% was from 27 kg to 66 kg. Greek nationality was confirmed by 97.8% of the respondents, while 2.1% answered another. The age of fathers who answered the questionnaire was 35–45 years for 65.2%, older than 46 years for 31.74%, and from 25–34 years for 3.04%. Mothers’ ages were 35–45 years for 76.9% of the sample, older than 46 years for 13%, and 25–34 years for 10%. Incomes from EURO 9001 to 25,000 were reported for 40.4% of the sample, 22.61% replied they earned more than EURO 25,000, while a high percentage gave no response.
A level of higher education was reported by 40.8% of the respondents, 20% had a master’s degree, and 6.9% had a doctorate, with 20.4% of respondents having a high school education, while a very small percentage of 2 in 270 responded below high school. Daily swimming pool use was reported by 23.4% of respondents, 71.3% used it 1 to 3 times a week, 4.7% answered occasionally, and one in 270 answered never. For the question of whether the child had a disease history, 7 answered autoimmune diseases, 2 answered were asthma, and 221 answered something else. Anatomical ear abnormality was reported by only 1.3% of the sample. The use of cotton swabs was reported by 36.52% of the sample with a negative response provided by 63.46%. Episodes of otitis media were reported by 22.6% of respondents, while 77.3% responded negatively. Swimming pool hygiene was poor to moderate at 25.7%, posing a risk to swimmers. While the remaining 72.4% responded from good to excellent. The highest percentage was observed at very good with 27%.
The changing rooms had a more negative image than the pools as a response of poor or moderate had a high rate of 40% of the sample, with 21% responding good, 16.5% very good, 12.2% excellent, and 3.5% answered they did not know. Toilet hygiene according to respondents’ answers was not very good as a rating of poor or average was provided by 47%, good was answered by 20.8%, very good for 16.5%, and excellent for 12.1%.
The answer about chlorine odor in the pool was divided with 50.4% responding yes and 49.57% responding no. The frequency of chlorine odor being rarely was answered by 30% of the sample, often by 22.1%, very often by 9.57%, and 37.5% of the sample, who answered no to the previous question, answered something else to this question. To the question of whether the children showered before entering the pool, 79.1% responded positively while 20.8% answered negatively. Child health as rated by parents was very good for 80%, good for 19.1%, poor for 0.4%, and very poor for 0.4%. In response to whether there was any health problem, 17.4% answered yes and 82.53% answered negatively. To the question of how they dealt with health problems, 63.46% of the sample replied by going to the hospital, health center, or doctor, 34.3% called the doctor, self-care answered by 1.3%, and 0.87% something else. After the disease event, 17.39% did not wait to go to the health center, 73% waited for 1–3 days, 8.7% waited more than 3 days, and 0.87% waited for symptoms to change. Self-care otitis treatment was not followed by 95.22%, while 4.76% followed self-treatment. For the children with otitis, 53.85% received antibiotic treatment, 23.08% took drops, and 23.06% responded that they received both antibiotics and otic drops. During an episode of otitis, 73.06% responded that they stopped using the pool while 26.92% replied that they continued using the pool.
Help was sought by 96.06% of the cases with otitis, 3.92% answered negatively, 77.39% did not respond, 19.1% saw a private doctor, and 3.04% were hospitalized. Otitis treatment was successful according to the response of 94.23% of the sample while it was considered unsuccessful by 5.77% of respondents. Recovery time was 4–7 days for 44.23%, 1–3 days for 42.31%, and more than 7 days for 13.46%.
3.4. Correlations
Lastly, through the correlation analysis, otitis could result from swimming in the pools. The most significant factor relating to otitis episodes was the frequency of swimmers’ use of the pool, which was statistically significant (n = 230, p = 0.021). Gender, weight, and age did not appear to affect the incidence and number of otitis media that resulted from the use of the pools. There was also no significant statistical relationship between locker rooms, toilets, and swimming pools with the episodes and the number of otitis rescued in the 4 swimming pools. Furthermore, chlorine odor and foreign bodies had no statistically significant relationship with otitis episodes. In addition, some abnormalities in the ear or the history of the child did not appear to affect the episodes of otitis (Table 2).
4. Discussion
Some microorganisms have been used as indicators to monitor the swimming pools. P. aeruginosa for instance, is used as an indicator organism for disinfection efficiency, while Escherichia coli is used as a fecal indicator. These microorganisms have some specific characteristics and are usually present at higher concentrations than pathogens, therefore, they are used as indicators. There are also publications that indicate that the presence of E. coli is strongly associated with P. aeruginosa [21]. Furthermore, the analysis methods are easier to apply and low-cost. These potential pathogens enter the pool (for instance by vomiting, saliva, mucus, and sweat), so there is a contingent health risk [22].
The main microbial agent responsible for external otitis media in children using swimming pools is Pseudomonas aeruginosa [23]. This germ can form biofilms on all surfaces and survive in treated water with residual chlorine levels < 1 mg/L. Therefore, contamination of swimming pool water is associated with outbreaks caused by P. aeruginosa [24,25]. The results of the microbiological quality of pools investigation revealed that all swimming pools had bacterial isolates. Our results are in agreement with a study conducted in 2016 on the bacteriological quality of swimming pool water in Port Harcourt Metropolis, in which Staphylococcus was the dominant microorganism identified [26]. Additionally, P. aeruginosa was present in all swimming pools, as well.
In terms of microbiological quality of water, according to Greek Standards Regulation 443/B/1974 for total coliforms, the sample should contain less than 15 cfu/100 mL. P. aeruginosa and S. auerus are not included in the Greek regulation, but they are considered indicators of water quality. In contrast, in German regulations (DIN 19643/1984) and the British Standards (BSI PAS 39:2003), E. coli should not be detectable at 100 mL. Total heterotrophic counts according to German regulation (DIN 19643/1984) should be less than 100 cfu/mL. In the Greek Standards Regulation 443/B/1974, total heterotrophic counts should be less than 200 cfu/mL. E. coli according to Greek Standards Regulation should be 0 cfu/100 mL.
Based on our results of the current study and according to Greek Regulations, all swimming pools were contaminated with microorganisms such as S. aureus and P. aeruginosa. This can be explained by the fact that practices regarding maintenance and hygiene requirements were inadequate and there is an urgent need for these measures to be upgraded [27]. For instance, these indicators for water quality should be included in the Greek Regulations [28]. Regarding the results of the microbiological analysis of water, swimming pools were not proper for swimming and, therefore, decontamination treatment and maintenance of pH at an optimum range were suggested. Additionally, examination of pool water quality on a constant basis is proposed as a preventive measure for monitoring potential health risks.
Moreover, excluding the microbiological analysis of the water, the US Centers for Disease Control and Prevention (CDC) suggests that the pH of the water should be from 7.2–7.8. More specifically, according to CDC, the residual chlorine concentration should be from 1–10 mg/L in the water at aquatic venues (other than hot tubs/spas) that do not use stabilized chlorine, or 2–10 mg/L when stabilized chlorine is used. Most bacteria and viruses get inactivated in water containing 1 mg/L of residual chlorine within minutes [19]. Although disinfection strategies were proposed to minimize potential health risks in swimming pools, the microbiological analysis of water showed it was still contaminated. Resistant strains can grow and multiply in the water even after treatment with antimicrobial agents [29]. In addition, the level of free residuals of chlorine in the swimming pool may not be proper and in compliance with the regulation standards. Furthermore, according to Blevins et al., 2004, when the tube that feeds the pool with chlorine is obstructed, there are more cases of acute gastroenteritis in children. Some other researchers have referred to diarrheal illness in swimming pools, as the levels of chlorination are not capable of killing some resistant viruses [30,31]. As for the pool water temperature, it should not be more than 25 °C. The air temperature around the pool must not be more than 5 °C warmer or/and 1 °C cooler than the temperature of the pool water [32].
The most important issue with the recreational water is that diseases affect not only developing countries but also developed ones [33,34,35]. Another grave problem with the recreational water is the use of chlorine which is the most commonly used chemical for disinfecting swimming pools [36]. There are studies that prove that chlorine chemical treatment provokes transformations in the permeability of lung epithelium via the skin and the eyes [37,38,39]. Therefore, it is imperative that chlorine should not exceed the prescribed limits. Although these factors were not statistically significant in this study, they remain crucial in terms of pool security issues [24].
Our study results showed a statistically significant factor (p = 0.021) for otitis incidents and the frequency of swimmers’ use of the pool. Our results are in agreement with a study that indicates risk factors for otitis externa are the frequency and duration of exposure to swimming pool water [40]. This can be explained by the fact that humans are not aquatic beings, so prolonged use of the pool seems to affect susceptibility to otitis due to the increase in the humidity in the outer auditory canal. Moreover, the conversion of pH of the external auditory canal to alkaline by destroying the protective effect of the cellular plug (that keeps the pH of the auditory channel acid) could be considered an additional vulnerability and transition factor to chronic external otitis. Therefore, it is highly recommended, that earbuds, cotton-tipped swabs, or anything that could irritate the ear should be avoided [41]. Although the treatment of otitis can be managed at the primary care level with simple procedures such as ear cleaning, there is an urgent need to upgrade the existing preventive measures in terms of public health [42].
5. Conclusions
Otitis externa is one of the most common childhood illnesses. This study focused on the risk of otitis externa in children who swim in pools. The most significant factor linking otitis episodes, according to the findings, is the frequency of swimmers’ use of the pool, which is statistically significant (n = 230, p = 0.021), as previously mentioned. In conclusion, it appears that the pool’s microbial load is not always linked to the occurrence of otitis. Because of the foregoing, using the pool should be done with caution. More research is needed to determine whether infections are truly linked to microbial load or if other factors are responsible for the spread of waterborne infections.
Author Contributions
Conceptualization, G.P. and A.V.; methodology, C.K.; software, J.V.; validation, G.P., J.V. and A.V.; investigation, G.P.; data curation, M.D.; writing—original draft preparation, G.P. and J.V.; writing—review and editing, M.D.; visualization, G.P. and A.V.; supervision, M.D. and A.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Smith, H. Swimmer’s ear: Prevention and Treatment. S. Afr. Pharm. Assist. 2019, 19, 19–20. [Google Scholar]
- Caramia, G.; Serafini, V.; Loggi, A. L’otite del nuotatore. Attualità e proposta preventiva. Pediatr. Med. Chir. 2013, 35, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Neghab, M.; Amiri, F.; Soleimani, E.; Hosseini, S.Y. The effect of exposure to low levels of chlorine gas on the pulmonary function and symptoms in a Chloralkali unit. J. Res. Health Sci. 2016, 16, 41–45. [Google Scholar] [PubMed]
- Martins, M.T.; Sato, M.I.Z.; Alves, M.N.; Stoppe, N.C.; Prado, V.M.; Sanchez, P.S. Assessment of microbiological quality for swimming pools in South America. Water Res. 1995, 29, 2417–2420. [Google Scholar] [CrossRef]
- Leclerc, H.; Schwartzbrod, L.; Dei-Cas, E. Microbial Agents Associated with Waterborne Diseases. Crit. Rev. Microbiol. 2002, 28, 371–409. [Google Scholar] [CrossRef]
- Wei, X.; Li, J.; Hou, S.; Xu, C.; Zhang, H.; Atwill, E.R.; Li, X.; Yang, Z.; Chen, S. Assessment of Microbiological Safety of Water in Public Swimming Pools in Guangzhou, China. Int. J. Environ. Res. Public Health 2018, 15, 1416. [Google Scholar] [CrossRef] [Green Version]
- WHO. Organizzazione Mondiale della Sanità 2006; World Health Organization: Geneva, Switzerland, 2006; Volume 2. [Google Scholar]
- Alhamlan, F.S.; Al-Qahtani, A.A.; Al-Ahdal, M.N. Recommended advanced techniques for waterborne pathogen detection in developing countries. J. Infect. Dev. Ctries. 2015, 9, 128–135. [Google Scholar] [CrossRef] [Green Version]
- Aboulfotoh Hashish, N.M.; Gawad Abbass, A.A.; Khamis Amine, A.E. Pseudomonas aeruginosa in swimming pools. Cogent Environ. Sci. 2017, 3, 1328841. [Google Scholar] [CrossRef]
- Mena, K.D.; Gerba, C.P. Risk Assessment of Pseudomonas aeruginosa in Water. In Reviews of Environmental Contamination and Toxicology; Springer: Boston, MA, USA, 2009; pp. 71–115. [Google Scholar] [CrossRef]
- Reid, T.M.S.; Porter, I.A. An outbreak of otitis externa in competitive swimmers due to Pseudomonas aeruginosa. J. Hyg. 1981, 86, 357–362. [Google Scholar] [CrossRef] [Green Version]
- Jayakar, R.; Sanders, J.; Jones, E. A study of acute otitis externa at Wellington Hospital, 2007–2011. Australas. Med. J. 2014, 7, 392–399. [Google Scholar] [CrossRef]
- Villedieu, A.; Papesh, E.; Weinberg, S.E.; Teare, L.; Radhakrishnan, J.; Elamin, W.F. Seasonal variation of Pseudomonas aeruginosa in culture positive otitis externa in South East England. Epidemiol. Infect. 2018, 146, 1811–1812. [Google Scholar] [CrossRef] [Green Version]
- He, E.; de Potter, P.; Shields, C.L.; Shields, J.A. Clinical variations of trilateral retinoblastoma: A re- port of 13 cases. J. Pediatr. Ophthalmol. Strabismus 2011, 129, 365–368. [Google Scholar]
- Lieberthal, A.S.; Carroll, A.E.; Chonmaitree, T.; Ganiats, T.G.; Hoberman, A.; Jackson, M.A.; Joffe, M.D.; Miller, D.T.; Rosenfeld, R.M.; Sevilla, X.D.; et al. The diagnosis and management of acute otitis media. Pediatrics 2013, 131, e964–e999. [Google Scholar] [CrossRef] [Green Version]
- Dufour, A.P.; Behymer, T.D.; Cantú, R.; Magnuson, M.; Wymer, L.J. Ingestion of swimming pool water by recreational swimmers. J. Water Health 2017, 15, 429–437. [Google Scholar] [CrossRef] [Green Version]
- Yedeme, K.; Legese, M.H.; Gonfa, A.; Girma, S. Assessment of Physicochemical and Microbiological Quality of Public Swimming Pools in Addis Ababa, Ethiopia. Open Microbiol. J. 2017, 11, 98–104. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, J.C.; Tucker, A.S. Development and Integration of the Ear. Curr. Top. Dev. Biol. 2015, 115, 213–232. [Google Scholar] [CrossRef]
- Murphy, J.L.; Hlavsa, M.C.; Carter, B.C.; Miller, C.; Jothikumar, N.; Gerth, T.R.; Beach, M.J.; Hill, V.R. Pool water quality and prevalence of microbes in filter backwash from metro-Atlanta swimming pools. J. Water Health 2018, 16, 93–101. [Google Scholar] [CrossRef] [Green Version]
- Saba, C.K.S.; Tekpor, S.K. Water Quality Assessment of Swimming Pools and Risk of Spreading Infections in Ghana. Res. J. Microbiol. 2015, 10, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Januário, A.P.; Afonso, C.N.; Mendes, S.; Rodrigues, M.J. Faecal indicator bacteria and pseudomonas aeruginosa in marine coastal waters: Is there a relationship? Pathogens 2020, 9, 13. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.C.; Keuten, M.G.; Knezev, A.; van Loosdrecht, M.C.; Vrouwenvelder, J.S.; Rietveld, L.C.; de Kreuk, M.K. Characterization of the bacterial community in shower water before and after chlorination. J. Water Health 2018, 16, 233–243. [Google Scholar] [CrossRef]
- Roland, P.S.; Stroman, D.W. Microbiology of acute otitis externa. Laryngoscope 2002, 112, 1166–1177. [Google Scholar] [CrossRef] [Green Version]
- Rice, S.A.; van den Akker, B.; Pomati, F.; Roser, D. A risk assessment of Pseudomonas aeruginosa in swimming pools: A review. J. Water Health 2012, 10, 181–196. [Google Scholar] [CrossRef] [Green Version]
- Roser, D.J.; van den Akker, B.; Boase, S.; Haas, C.N.; Ashbolt, N.J.; Rice, S.A. Pseudomonas aeruginosa dose response and bathing water infection. Epidemiol. Infect. 2014, 142, 449–462. [Google Scholar] [CrossRef]
- Amala, S.E.; Aleru, C.P. Bacteriological Quality of Swimming Pools Water in Port Harcourt Metropolis. Nat. Sci. 2016, 8, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Saberianpour, S.; Momtaz, H. Assessment of Bacterial and Fungal Contamination in Public Swimming Pools in Shahrekord—Iran. J. Trop. Dis. 2016, 4, 2–5. [Google Scholar] [CrossRef]
- Tirodimos, I.; Christoforidou, E.P.; Nikolaidou, S.; Arvanitidou, M. Bacteriological quality of swimming pool and spa water in northern Greece during 2011–2016: Is it time for Pseudomonas aeruginosa to be included in Greek regulation? Water Sci. Technol. Water Supply 2018, 18, 1937–1945. [Google Scholar] [CrossRef]
- Papadopoulou, C.; Economou, V.; Sakkas, H.; Gousia, P.; Giannakopoulos, X.; Dontorou, C.; Filioussis, G.; Gessouli, H.; Karanis, P.; Leveidiotou, S. Microbiological quality of indoor and outdoor swimming pools in Greece: Investigation of the antibiotic resistance of the bacterial isolates. Int. J. Hyg. Environ. Health 2008, 211, 385–397. [Google Scholar] [CrossRef]
- Keswick, B.H.; Satterwhite, T.K.; Johnson, P.C.; DuPont, H.L.; Secor, S.L.; Bitsura, J.A.; Gary, G.W.; Hoff, J.C. Inactivation of Norwalk virus in drinking water by chlorine. Appl. Environ. Microbiol. 1985, 50, 261–264. [Google Scholar] [CrossRef] [Green Version]
- Podewils, L.J.; Blevins, L.Z.; Hagenbuch, M.; Itani, D.; Burns, A.; Otto, C.; Blanton, L.; Adams, S.; Monroe, S.S.; Beach, M.J.; et al. Outbreak of norovirus illness associated with a swimming pool. Epidemiol. Infect. 2007, 135, 827–833. [Google Scholar] [CrossRef]
- Neghab, M.; Gorgi, H.A.; Baghapour, M.A.; Rajaeefard, A.; Moemenbellah-Fard, M.D. Bacterial Contamination of the Swimming Pools in Shiraz, Iran; Relationship to Residual Chlorine and Other Determinants. Pak. J. Biol. Sci. 2006, 9, 2473–2477. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Global Water, Sanitation and Hygiene; World Health Organization: Geneva, Switzerland, 2018; p. 52. Available online: https://www.who.int/water_sanitation_health/publications/global-water-sanitation-and-hygiene-annual-report-2018/en/ (accessed on 8 February 2022).
- Giampaoli, S.; Spica, V.R. Health and safety in recreational waters. Bull. World Health Organ. 2014, 92, 79. [Google Scholar] [CrossRef] [PubMed]
- Mavridou, A.; Pappa, O.; Papatzitze, O.; Dioli, C.; Kefala, A.M.; Drossos, P.; Beloukas, A. Exotic Tourist Destinations and Transmission of Infections by Swimming Pools and Hot Springs—A Literature Review. Int. J. Environ. Res. Public Health 2018, 15, 2730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, S.D.; DeMarini, D.M.; Kogevinas, M.; Fernandez, P.; Marco, E.; Lourencetti, C.; Ballesté, C.; Heederik, D.; Meliefste, K.; McKague, A.B. What’s in the pool? A comprehensive identification of disinfection by-products and assessment of mutagenicity of chlorinated and brominated swimming pool water. Environ. Health Perspect. 2010, 118, 1523–1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Luna, Á.; Burillo, P.; Felipe, J.L.; Gallardo, L.; Tamaral, F.M. Chlorine concentrations in the air of indoor swimming pools and their effects on swimming pool workers. Gac. Sanit. 2013, 27, 411–417. [Google Scholar] [CrossRef] [Green Version]
- Zarzoso, M.; Llana, S.; Pérez-Soriano, P. Potential negative effects of chlorinated swimming pool attendance on health of swimmers and associated staff. Biol. Sport 2010, 27, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Dalmau, G.; Estela Martínez-Escala, M.; Gázquez, V.; Pujol-Montcusí, J.A.; Canadell, L.; Espona Quer, M.; Pujol, R.M.; Vilaplana, J.; Gaig, P.; Giménez-Arnau, A. Swimming pool contact dermatitis caused by 1-bromo-3-chloro-5,5-dimethyl hydantoin. Contact Dermat. 2012, 66, 335–339. [Google Scholar] [CrossRef]
- Kujundžić, M.; Braut, T.; Manestar, D.; Cattunar, A.; Malvić, G.; Vukelić, J.; Pušelja, Ž.; Tomić Linšak, D. Water related otitis externa. Coll. Antropol. 2012, 36, 893–897. [Google Scholar]
- Khosravani, M.; Abedi, H.A.; Lak, S.; Rafiei, F.; Rahzani, K. The association between conscience understanding and clinical performance among nurses working at education hospital of Arak. Ann. Trop. Med. Public Health 2017, 10, 1587–1590. [Google Scholar] [CrossRef]
- Marais, A. Clinical evidence in the management of swimmer’s ear. S. Afr. Fam. Pract. 2015, 57, 4–8. [Google Scholar]
Figure 1.
Study design.


{kind=link}
Table 1.
Average microbial analysis in pools (cfu/100 mL).
| E. coli Average | S. aureus Average | Coliforms Average | Aerobic Microorganisms Average | P. aeruginosa Average | |
|---|---|---|---|---|---|
| Limits | 0 | 0 | 15 | 200 | 0 |
| SP1 | 0 | 9.2 | 2.9 | 44.8 | 4.4 |
| SP2 | 0 | 9 | 0 | 29.5 | 4 |
| SP3 | 0.7 | 22.6 | 7 | 82.1 | 10.3 |
| SP4 | 0.3 | 12.2 | 2 | - | 18.5 |
Table 2.
Correlations between the questions and p-value.
| Correlations | p-Value |
|---|---|
| 1. Swimming pool name * recovery time | 0.452 |
| 2. Swimming pool name * episodes of otitis | 0.432 |
| 3. Child history * episodes of otitis | 0.255 |
| 4. Child history * recovery time | 0.401 |
| 5. Family income * episodes of otitis | 0.654 |
| 6. Anatomical ear abnormality * episodes of otitis | 0.655 |
| 7. Anatomical abnormal ear * recovery time | 0.354 |
| 8. Gender * episodes of otitis | 0.431 |
| 9. Gender * number of episodes of otitis | 0.398 |
| 10. Age * episodes of otitis | 0.057 |
| 11. Age * number of episodes of otitis | 0.167 |
| 12. Weight (kg) * episodes of otitis | 0.125 |
| 13. Weight (kg) * number of episodes of otitis | 0.189 |
| 14. Frequency of use of the pool * episodes of otitis | 0.021 |
| 15. Pool hygiene * episodes of otitis | 0.333 |
| 16. Pool hygiene * number of episodes of otitis | 0.401 |
| 17. Locker room hygiene * episodes of otitis | 0.541 |
| 18. Locker room hygiene * number of episodes of otitis | 0.449 |
| 19. Toilet hygiene * episodes of otitis | 0.438 |
| 20. Toilet hygiene * number of episodes of otitis | 0.522 |
| 21. Health of child * episodes of otitis | 0.351 |
| 22. Health of child * number of episodes of otitis | 0.255 |
| 23. Educational level * episodes of otitis | 0.302 |
| 24. Usage of cotton swabs * episodes of otitis | 0.741 |
| 25. Intense chlorine odor * episodes of otitis | 0.228 |
| 26. Foreign bodies * episodes of otitis | 0.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Pantazidou, G.; Dimitrakopoulou, M.; Kotsalou, C.; Velissari, J.; Vantarakis, A. Risk Analysis of Otitis Externa (Swimmer’s Ear) in Children Pool Swimmers: A Case Study from Greece. Water 2022, 14, 1983. https://doi.org/10.3390/w14131983
AMA Style
Pantazidou G, Dimitrakopoulou M, Kotsalou C, Velissari J, Vantarakis A. Risk Analysis of Otitis Externa (Swimmer’s Ear) in Children Pool Swimmers: A Case Study from Greece. Water. 2022; 14(13):1983. https://doi.org/10.3390/w14131983
Chicago/Turabian StylePantazidou, G., ME. Dimitrakopoulou, C. Kotsalou, J. Velissari, and A. Vantarakis. 2022. "Risk Analysis of Otitis Externa (Swimmer’s Ear) in Children Pool Swimmers: A Case Study from Greece" Water 14, no. 13: 1983. https://doi.org/10.3390/w14131983
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.