
Abstract
Previous reviews have often shown a link between digital media ADHD symptom levels. However, longitudinal studies are needed to find stronger evidence of a causal effect as well as to determine the direction of effects. The aim of the present review (PROSPERO CRD42021262695) was therefore to provide a systematic review of studies meeting the following inclusion criteria: (1) include longitudinal data investigating associations between digital media (i.e., gaming and social media) and later ADHD symptoms or vice versa, (2) be published within the past 10 years (i.e., 2011 until June 2021), (3) be published in a peer-reviewed journal in English, and (4) include children or adolescents (age 0–17 years). After a systematic search in the Web of Science and PsycInfo databases, we included 28 studies, all with adequate or high quality. Results showed support for reciprocal associations between digital media and ADHD symptoms, with associations being more consistent for problematic use of digital media than for screen time. Thus, children with ADHD symptoms appear more vulnerable to developing high or problematic use of digital media (i.e., selection effects), and digital media also have effects on later ADHD symptom levels, either because of specific characteristics of digital media or because of indirect effects on, for example, sleep and social relations (i.e., media effects). However, it should be emphasized that further studies investigating potential moderators and mediators are needed if we are to better understand the complex associations between digital media and ADHD symptom levels.
Similar content being viewed by others


Introduction
Today, almost all teenagers in Western countries have their own smartphone [1], and the time spent using digital media (i.e., any activity that uses a digital device for leisure purposes such as playing digital games, using social media, or taking part of information or entertainment on the Internet) has increased radically during the past decade [2]. At the same time as children’s access to digital media has increased greatly, there has also been a large increase in the number of children diagnosed with Attention Deficit Hyperactivity Disorder (ADHD) [3]. This has led to the concern that digital media use might have effects on ADHD symptom levels. There are now several reviews and meta-analyses investigating the link between digital media in general and ADHD [4, 5], as well as more specific reviews focusing on the link between gaming and ADHD [6, 7] or ADHD symptom levels for individuals diagnosed with Internet gaming disorder [8, 9]. However, because this is an extremely fast-moving research area, there is a need for a new review that captures the current state of the field. In addition, none of the available reviews addressing this area has focused specifically on longitudinal relations. Longitudinal studies have the great advantage of being able to control for baseline levels and, thereby, to investigate to what extent digital media use influences changes in ADHD symptoms levels over time. It should also be noted that the association between digital media and mental health is most likely characterized by reciprocal relations in which both constructs affect each other over time [10], and longitudinal studies are able to investigate the direction of the effects. The overall aim of the present study was therefore to conduct a systematic review of longitudinal studies investigating the association between digital media and ADHD symptoms and vice versa.
Digital media addiction
Previously, problematic media use has often been defined as entailing exposure to violent media content, whereas recent studies have focused more on the overarching negative consequences of digital media use. One important reason for this shift is most likely the introduction of “Gaming Disorder” (GD) in the 11th edition of the International Classification of Disease (ICD-11) [11] and “Internet Gaming Disorder” (IGD) as a diagnosis in need of further validation in the 5th edition of the Diagnostical and Statistical Manual of Mental Disorders (DSM-5) [12]. IGD includes nine different symptom criteria: (1) preoccupation with gaming, (2) withdrawal symptoms when gaming is taken away, (3) tolerance, (4) unsuccessful attempts to control gaming, (5) loss of interest in previous hobbies/activities as a result of gaming, (6) continued gaming despite psychosocial problems, (7) deception, (8) gaming to escape or relieve negative mood, and (9) jeopardizing relationships, job, or educational/career opportunities because of gaming.
Thus far, there has been no official recognition of addictive social media usage in DSM-5. However, it has been argued that criteria similar to those described above for IGD can also be applied to social media use [13,14,15,16]. It has also been suggested that a Social Media Disorder (SMD) should be included as a psychiatric disorder in the next version of the DSM, the argument being that social media use can be just as addictive and have just as serious effects on mental health as excessive gaming [16,17,18,19]. The current review is therefore not limited to gaming.
Hypotheses linking digital media use and ADHD symptoms
Several hypotheses have been presented to explain how digital media use could be related to ADHD symptoms or vice versa. Some of these effects might apply to more general associations between digital media use and mental health problems, whereas some hypotheses focus on why digital media use might be associated with ADHD in particular. In addition, some of these hypotheses focus on explaining why digital media use can lead to increased levels of ADHD symptoms (i.e., media effects), whereas others focus on why children with ADHD symptoms might be more likely to develop problematic use of digital media later on (i.e., selection effects). It is important to emphasize that different hypotheses are not mutually exclusive—all of them could be correct to some degree, and they may also differentially explain the process on an individual level. It should also be noted that we can only speculate regarding this as randomized control trials (RCT), the best design for making causal inferences, is not possible to use within this area of research as few individuals are willing to refrain from using digital media. Experimental studies (e.g., ecological momentary assessment where the participant responds to a few questions several times per day) can provide much valuable information but are cumbersome to undertake as effects of digital media on ADHD symptom levels require relatively long study periods, and this design would therefore be overly intrusive in a person’s life.
One initial hypothesis is that the association between digital media use and ADHD symptoms represents a direct causal effect (i.e., something in the digital media content is directly causing symptoms of inattention, hyperactivity, and impulsivity). The “scan and shift hypothesis” [20] states that the fast pace of digital media may encourage using attentional resources to quickly scan and shift, making it more difficult to later engage in tasks requiring sustained attention. In addition, it has been hypothesized that children who have high levels of screen time have a harder time paying attention to less interesting activities, possibly because they lose the ability to regulate their attention internally after having gotten used to external regulation through digital media [21]. Violent media content has also been linked to ADHD symptoms, most likely because violent media are high in arousal, and the characters in this type of media often act impulsively [22]. It has also been shown that media multitasking is related to inattention, the hypothesis being that individuals engaged in media multitasking have difficulties focusing on one task, because they are accustomed to task-switching between media activities and other (offline or online) activities [23].
As described above, digital media use may have effects on ADHD symptoms, because such use leads to high arousal, which in turn leads to habituation and difficulties performing activities that are low in arousal. However, it should be noted that the direction of these effects is still unclear, as most studies have investigated cross-sectional correlations. According to the “Differential susceptibility to media effects model” [24], individuals are likely to select media content that fits within their existing dispositions. With regard to ADHD, it has been suggested that individuals with this disorder are more attracted than others to fast-paced activities, creating high arousal and delivering immediate rewards [5, 25]. Individuals with ADHD also often have problematic peer relations [e.g., 26] and show poor academic achievement [e.g., 27]. They may therefore use digital media as an escape from both reality and the negative feelings of being rejected, which in turn predicts the development of problematic digital media use as well as other mental health problems. Thus, escapism can be both a predictor of IGD and a mediator between digital media use and poor mental health [review by 28]. Of importance here is also the “social compensation hypothesis,” which states that individuals with poor social networks offline try to compensate for this by focusing more on online relations [e.g., 29]. In summary, children with ADHD symptoms may be more prone than other children to develop digital media addictions, with some individuals (e.g., those with poor social relations) being at particularly high risk. In addition, and as emphasized above, the links between ADHD and digital media use are likely reciprocal. This is sometimes referred to as the “Reinforcing Spiral Model” [10], which indicates that individuals with, for example, ADHD choose specific media content that is in line with their prevailing predisposition, which in turn may reinforce problematic behaviors.
In addition to direct causal effects of digital media use on ADHD symptom levels, it has been proposed that indirect causal effects could also be important. This hypothesis is sometimes referred to as the displacement hypothesis, as it suggests that time spent on digital media crowds out health-promoting behaviors, which in turn could increase ADHD symptom levels. Two of the most important activities commonly affected by extensive use of digital media are physical activity [e.g., reviews 30, 31] and sleep [e.g., 32]. In addition, excessive use of digital media early in life has been shown to be associated with lower levels of social interaction [e.g., 33] and delayed speech development [e.g., 34], which in turn can have a negative impact on peer relations. Thus, digital media use can affect several different health-promoting activities. These health-promoting activities are also linked to ADHD symptoms [35], and excessive use of digital media might therefore amplify pre-existing difficulties with maintaining unhealthy behaviors that children and adolescents with ADHD may already display due to the nature of their diagnosis. This could indicate that a small decrease in health-promoting behaviors has a larger negative impact on children with ADHD, because they start out at a lower level than their peers do. In the present review, we will therefore discuss to what extent the associations between ADHD and digital media use are affected by baseline levels (i.e., what level of problem behaviors or health-promoting behaviors the child already has), as well as to what extent effects of ADHD symptoms on later digital media use, or vice versa, are linear or non-linear.
Fourth, there is also a possibility that the observed association between digital media and ADHD symptoms is spurious and caused by a third variable, such as low socioeconomic status or male sex, factors known to be strongly associated with both ADHD and digital media use [4]. The present review will therefore provide an overview of the effects of different covariates.
Results of previous reviews and meta-analyses
Although there are, thus far, no reviews of longitudinal studies examining the link between digital media use and ADHD symptoms, some previous reviews and meta-analyses including primarily concurrent data have provided valuable insights. Generally, the results of these studies show significant associations between ADHD symptoms and digital media use, but the strength of these relations varies greatly across studies depending on, for example, what type of sample has been studied and the type of digital media in focus. More specifically, several reviews [8, 9, 36, 37] have shown that there is an overrepresentation of ADHD among children/adolescents with problematic use of digital media (often defined as symptoms of IGD or Internet addiction). When investigating ADHD symptom levels rather than diagnosis, the results from previous reviews are less clear. Ferguson [6] concluded that computer gaming is not significantly associated with inattention, while another study [38] found an association between Internet use in general and ADHD symptom levels. Several previous reviews [4, 5, 22] have concluded that ADHD symptoms are significantly, but only weakly, associated with digital media use. However, this is most likely explained by the fact that many studies have controlled for different background variables (e.g., sex, age, SES, upbringing) in the statistical analyses rather than investigating their impact as moderators of the association of interest. This could suggest that there are subgroups of children with ADHD who are especially vulnerable to developing problematic use of digital media.
Aim of the present review
As described above, there are both several plausible hypotheses and empirical support suggesting an association between digital media use and ADHD symptoms. However, the relatively large number of studies conducted recently are not included in these previous reviews, because they were published only a few years back. In addition, no previous review has focused on longitudinal studies. The overall aim of the present study was therefore to conduct a systematic review of longitudinal studies published within the past 10 years and examining the link between ADHD symptoms and digital media use. More specifically, the present study reviewed the previous literature with regard to the following research questions:
-
1.
Is digital media use related to later ADHD symptom levels (i.e., media effects)?
-
2.
Are ADHD symptom levels related to later digital media use (i.e., selection effects)?
-
3.
In what way do covariates, mediators, and moderators influence the association between ADHD symptoms and digital media use and vice versa?
Methods
Search strategy
The updated Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) [39] was used during the review process. A comprehensive literature search was conducted using PsycInfo and Web of Science. Reference lists of retrieved articles and review papers were also examined for any further studies. The exact search words used are presented in Table 1. Each of the studies found in the search was systematically and independently reviewed by at least two of the authors. In case of disagreement between the two raters, a third author was consulted, and a consensus decision was made between the three raters. The review was registered in PROSPERO (CRD42021262695).
Inclusion and exclusion criteria
The inclusion criteria for papers to be reviewed were the following: (1) published within the past 10 years (i.e., 2011 until June 2021), (2) published in English, (3) published in a peer-reviewed journal, (4) including children or adolescents (age 0–17 years), and (5) using longitudinal data to investigate the relation between ADHD symptoms/diagnosis and digital media. Regarding the exclusion criteria, we did not include studies of children with ADHD recruited within a very limited setting (i.e., the criminal justice setting) or studies that only included children with ADHD and another comorbid medical or mental condition. In addition, we did not include the few available studies focusing exclusively on watching TV. The reason for this was that most children today do not watch digital media on a TV, but rather stream various types of digital media content (e.g., Netflix, YouTube) using several different platforms. For this reason, focusing on exclusively on TV watching does not capture the children’s digital media habits very well. We also excluded studies assessing ADHD symptoms using cognitive tasks (e.g., continuous performance tasks [CPT] to assess attention problems) as ratings and tests of inattention/impulsivity are not highly correlated and many tests of attention also measure other cognitive functions (e.g., speed of processing, working memory). Thus, including both ratings and tests would most likely have created too much heterogeneity.
Included studies
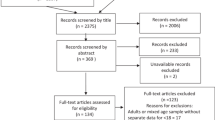
As shown in the flow chart presented in Fig. 1, a total of 586 references remained after removing duplicates. Of these, 533 reports were excluded based on the title and the information presented in the abstract. This left 53 reports for full-text screening. Out of these 53 reports, 25 were excluded, resulting in a total of 28 reports included in the review from altogether 25 different studies. The main reasons for exclusion of the report undergoing a full-text review were that the study (1) was not longitudinal (at least not for the analyses investigating relations between digital media and ADHD symptoms), (2) did not investigate ADHD symptoms specifically but rather a broader construct such as externalizing behavior problems, or (3) did not address digital media specifically but rather media use in general (e.g., reading books/magazines, listening to music).

Flowchart
The characteristics of the studies included in the review are presented in Table 2. Here, it is shown that the included studies varied in how they measured both ADHD symptoms and digital media. Most studies used some sort of ratings (self-reports, parent ratings, or teacher ratings), whereas three reports from the same project [40,41,42] used interviews to assess ADHD symptom levels and/or IGD symptoms. In addition, most studies (n = 19; 68%) used the same rater for both the predictor and the outcome measure, with 11 studies using only self-ratings and 8 studies using only parent ratings. For the studies using different raters at baseline and follow-up (n = 9), five studies used self-ratings to assess digital media use and parent ratings to assess ADHD symptom levels. The most used measures for assessing ADHD symptom levels (i.e., included in 23 out of 28 studies) were scales including the DSM-5 symptom criteria for ADHD (e.g., the ADHD rating Scale–IV) or the Strength and Difficulties Questionnaire (SDQ).
Quality ratings
Articles were assessed for quality utilizing the Quality Assessment Tool for Observational and Cohort and Cross-Sectional Studies created by the National Institutes of Health [43]. This scale includes 14 criteria and items related to internal validity, external validity, and study power. Each criterion was rated as 0 (i.e., criterion not met) and 1 (criterion met). Thus, the possible range was 0–14. Regarding Criterion 5 (i.e., power/sample size), an adequate power calculation or a sample size above 1000 participants at baseline was required for this criterion to be met. For Criterion 7 (i.e., sufficient time frame), we set the limit at 1 year for at least one of the follow-ups. Concerning Criterion 12 (i.e., blinding of outcomes assessors), we regarded this criterion as having been met if the outcome was assessed using an objective measure (i.e., interview) or if the study included separate raters for the predictor and outcome variable. For Criterion 13 (i.e., retention rate), we followed the recommendations and set the limit to at least 80%. A score of 0–6 was considered poor, 7–10 adequate, and 11–14 high quality. Two of the authors (LBT and JB) performed the quality ratings independently, and when necessary, reached a decision by consensus. However, it was only for criterion 13 (i.e., retention rate) that some inconsistencies between raters were found as this information was sometimes not very clearly described in the articles.
Results
Description of the included articles
As shown in Table 2, as many as 14 (50%) of the studies included in the review were published during 2020 or the first half of 2021, even though the time span for inclusion was the past 10 years. Many of the studies included large sample sizes (i.e., 17 studies with a sample size > 1000 at baseline), and the total number of participants at baseline in the studies was just above 66,000 taking into consideration that some of the studies were from the same project and therefore included the same individuals (see footnote in Table 2). Regarding the participants’ age, the studies included preschool children (n = 5), children aged 6–12 years (n = 9), or adolescents (n = 11), but a few studies included children from a larger age range (n = 3). The time span from baseline to follow-up ranged from 3 months to 8 years, with most studies using a follow-up period of about 1–2 years. It should be noted that all included studies examined symptom levels of inattention, impulsivity, and hyperactivity on a dimensional level (i.e., from low to high symptom levels) rather than focusing on ADHD diagnosis. All studies included between-subject effects and five studies [42, 44,45,46,47] also investigated within-subject effects. Most studies reported between-subject effects both with and without control for baseline levels (i.e., controlled for digital media use at baseline when examining associations between ADHD symptoms and later digital media use, or vice versa). However, four studies [48,49,50,51] failed to control for baseline levels altogether.
Regarding digital media use, the measures used in the studies included here can be classified into two broad categories: studies investigating screen time (i.e., time spent using some type of digital media) and studies investigating digital media addiction (i.e., excessive use and negative consequences of using digital media). Regarding screen time, the studies can also be classified into the following categories, with some studies including more than one type of digital media: digital media in general (n = 8), violent media (n = 3), gaming (n = 9), social media (n = 2), multitasking (n = 1), and cyberbullying/sexual exposure (n = 1). Regarding addiction, the included studies investigated Internet addiction in general (n = 3), gaming (n = 7), or social media (n = 1). An equal number of studies (19 out of 28) investigated digital media in relation to later ADHD symptom levels and the reverse relation. Thus, 10 of the included studies included reciprocal relations between digital media and ADHD symptoms. A brief description of how digital media and ADHD symptoms were assessed can be found in Table 2 (i.e., columns 2 and 3). In case a distinction was made between the different sub-symptoms of ADHD, this is clarified in the description of the results in column 6.
The quality ratings (QR) for the included studies are presented in the last column of Table 2. The total mean score on the quality assessment tool was 10.57, with scores ranging from 7 to 14. None of the included studies was considered to be of poor quality; 11 studies (39%) were of adequate quality and 17 studies (61%) were of high quality. Almost all studies met Criterion 1 (i.e., objectives and hypothesis) and Criterion 2 (i.e., study group description). In addition, all studies used reliable and valid measures of ADHD symptom levels, whereas only 16 studies (57%) provided information about the reliability of the measure used to assess digital media. Concerning Criterion 13 (i.e., retention rate), 16 studies (57%) had a retention rate of at least 80%. The lowest percentages were found for Criterion 10 (i.e., repeated exposures) with only 32% of the studies including more than two time-points and Criterion 11 (i.e., blinding), with only 36% of the studies using objective measures (i.e., interview) or different raters for the predictor and the outcome measures.
Overall findings
As shown in Table 2, many of the studies included in the present review found significant associations both of digital media use on later ADHD symptoms and of ADHD symptoms on later digital media use. However, it is important to note that sample sizes were often very large, which means that the power to detect even small effects was high. In general, the size of the effects was relatively small (see last column of Table 2). As the included studies used many different types of analyses and a range of different covariates, a comparison between studies is difficult. However, results indicated that associations between problematic use of digital media and ADHD symptoms were somewhat more common and were stronger than associations between screen time and ADHD symptoms. In the case of significant associations, they were always positive (i.e., high levels of digital media being associated with high ADHD symptom levels or vice versa). To provide an overview of the results, a summary is presented in Fig. 2. This figure shows that significant associations in both directions (i.e., digital media in relation to later ADHD symptom levels and vice versa) were almost always found when not controlling for baseline levels. A substantial proportion of the studies (i.e., 33–75%) also found significant associations in between-subject analyses when controlling for baseline levels, whereas within-subject analyses were uncommon and only a minority of available studies found significant associations. These findings are presented in more detail below.

Summary of the results displaying the number of studies showing significant associations between ADHD symptom levels and digital media (DM)
Digital media in relation to later ADHD symptom levels
Screen time
Regarding studies investigating screen time in general (i.e., often an aggregated measure of use of computers, game consoles, mobile phones, and TV), the results of the current review show that eight studies found significant positive associations with later ADHD symptom levels or with symptoms of inattention when controlling for baseline levels of screen time [44, 47, 52,53,54,55,56,57]. Beyens et al. [44] only found associations between overall media exposure and later ADHD symptoms in between-subject analyses and not in within-subject analyses. In addition, three studies [40, 48, 49] only found relations when not controlling for baseline levels. The review also includes two studies that failed to find any significant associations between screen time in general and later ADHD symptom levels. Of these studies, Niiranen et al. [58] investigated screen time in children as young as 18 months in relation to ADHD symptom levels at age 5, where the cutoff for excessive screen time was defined as more than 45 min/day. Paulain et al. [59], who included a sample of children aged 10–17 years, found significant associations between use of computers/Internet and several other outcomes (e.g., peer relations, well-being, and quality of life), but not for ADHD symptom levels.
In studies investigating screen time for violent media (usually violent computer games) and later ADHD symptom levels, one study failed to find a significant association [60], while another study [54] found a significant association, although it did not remain significant when controlling for ADHD symptom levels at baseline. A third study [44] found that screen time for violent media at Time 1 was not related to ADHD symptoms at Time 2. However, screen time for violent media at Time 2 was significantly related to ADHD symptom levels at Time 3, although not when controlling for earlier ADHD symptom levels.
With regard to more specific measures of screen time, McNamee et al. [45] found a significant relation between screen time for social media and later ADHD symptom levels in within-subject analyses, whereas Boer et al. [46] only found a significant association when not controlling for baseline levels of social media use. Finally, one study [47] found a significant association between screen time for media multitasking (i.e., using several different media simultaneously) and later ADHD symptom levels in between-subject but not in within-subject analyses.
Digital media addiction
Although studies investigating the association between digital media addiction and ADHD symptoms have grown in number during the past few years, only four of them were longitudinal. Hygen et al. [42] found that symptoms of IGD at age 10 years were related to ADHD symptom levels both 2 and 4 years later, although these associations were only found in the between-subject (with and without control for baseline levels) and not in the within-subject analyses. Wartberg et al. [61] also found a small association between symptoms of IGD and later ADHD symptom levels when controlling for baseline levels of IGD symptoms, whereas Ferguson & Ceranoglu [62] failed to find such a relation. Here, it should be noted that the latter study included a few participants (n = 144), the majority of whom did not display a single symptom of IGD. Finally, Boer et al. [46] found a significant association between problematic social media use and later symptoms of inattention and to some extent impulsivity, but not hyperactivity. Associations were found for both between-subject (with and without control for baseline levels) and within-subject analyses.
ADHD symptoms in relation to later digital media use
Screen time
Regarding ADHD symptom levels in relation to later screen time, seven studies found at least some significant associations, but only three studies found associations when controlling for ADHD symptom levels at baseline. Of the studies finding significant associations with control for baseline, Beyens et al. [44] found associations to screen time for violent media in both between-subject and within-subject analyses. In addition, Stenseng et al. [40] found that ADHD symptoms at age 6 were related to time spent on computer gaming at age 8. However, ADHD symptoms at age 8 were not related to time spent on computer gaming at age 10. Finally, Gentile et al. [54] found that attention problems were related to later video game playing. The studies that failed to find associations when controlling for ADHD symptom levels at baseline (or failed to control for baseline levels altogether) investigated screen time in general [51, 63, 64], screen time for multitasking [47], social media [46], violent games [50], and Internet bullying/sexual harassment [64].
Digital media addiction
Regarding studies examining associations between ADHD symptoms and later gaming addiction, all studies except three [41, 42, 46] found significant relations [61,62,63, 65,66,67], when controlling for baseline levels. In addition, Hirota et al. [68] found that inattention, but not hyperactivity, was associated with both the persisting pattern (i.e., stability of Internet addiction across time) and the converting pattern (i.e., from no Internet addiction to Internet addiction) across 2 years. Interestingly, two studies [41, 42] not finding significant associations when controlling for baseline levels used interviews to assess gaming addiction. The only study [46] investigating ADHD symptoms in relation to later social media addiction only found significant associations when not controlling for baseline levels of ADHD symptoms. It should also be noted that several studies found that the association between early ADHD symptoms and later gaming addiction did not remain significant when many covariates were included (e.g., age, child sex, family functioning, academic achievement, pregnancy factors, aggression, and self-esteem; see Table 2 for details).
Reciprocal associations
A total of ten studies investigated reciprocal associations. Although these studies are included in the results section above, we mention them again here, because they used a design which provided information about the directionality of the associations. A summary of these studies showed that when controlling for baseline levels, three studies found support for bi-directional associations between digital media use and ADHD symptoms [44, 54, 61], four studies found unidirectional associations between digital media use and later ADHD symptoms [42, 46, 47, 56], two studies found unidirectional associations between ADHD symptoms and later digital media use [40, 62], and one study did not find any significant associations [59].
Covariates, mediators and moderators
Effects of sex and age
As most studies included in this review used sex as a covariate rather than as a moderator, we still do not know to what extent the association between digital media use and ADHD symptom levels is stronger for boys than for girls or vice versa. However, Baumgartner et al. [47] showed that the relation between media multitasking and later ADHD symptom levels was twice as large for girls as for boys, and Rydell and Brocki [50] found that symptoms of inattention predicted violent media use 1 year later for boys only. Finally, one study [56] failed to find a moderating effect of sex.
Regarding effects of age, only one study [56] conducted a proper moderation analysis, and it failed to find a moderating effect of age in a sample of children aged 2–6 years when examining screen time in relation to later ADHD symptoms and vice versa. In addition, five studies examined to what extent the association was significant in one age group and not in another. Allen et al. [52] found that screen time was only related to later ADHD symptom levels at age 10 and not age 6. In addition, Baumgartner et al. [47] found an effect of multitasking on later inattention only for children 11–13 years of age and not for teenagers 13–15 years. Hygen et al. [42] found that gaming addiction at age 10 was related to ADHD symptom levels at both age 12 and 14. Liu et al. [49] found that screen time at both 6 months and 2.5 years was related to ADHD symptom levels at age 4. Finally, Stenseng et al. [40] found that ADHD symptom levels at age 6 were associated with screen time at age 10, but that ADHD symptom levels at age 10 were not significantly associated with screen time at age 12. In conclusion, the results are very mixed, and there is little evidence to support the claim that effects are generally stronger for a specific age.
Additional variables
As shown in Table 2, the studies included in this review included a large range of different covariates in addition to age and sex. For example, Allen et al. [52] showed no moderating effect of parental income, pubertal status and upbringing, and Hetherington et al. [48] found no moderating effect of either hostile/ineffective parenting or positive parenting. Both these two studies examined the association between screen time for video games/TV and later ADHD symptoms. However, Peeters et al. [66] found that the effect of attention problems in relation to later symptoms of IGD was stronger for adolescents who had fewer close relationships and who were less satisfied with life.
Regarding mediators and covariates, there are studies showing that only the effects of school performance and peer problems [63] or sleep problems [53] remained significant when investigating the association between digital media use and later ADHD symptoms. Finally, Jeong et al. [65] showed support for a mediating effect of low self-esteem for both boys and girls and aggression for girls when investigating the relation between ADHD symptoms and later symptoms of IGD. None of the studies investigated underlying neuropsychological deficits (e.g., executive functioning, emotion regulation, or reward sensitivity) as possible mediators in the association between digital media and ADHD symptom levels.
It should also be noted that other studies included in the present review included a very large range of control variables. These include family climate, intelligence, child temperament, emotion regulation, passive smoking, outdoor activities, school performance, self-esteem, pregnancy factors, executive functioning, physical activity, and social skills (see Table 2 for details). The relation between digital media use and ADHD symptom levels generally disappeared when including a large range of covariates, which indicates that at least some of these factors are of importance. However, because these control variables were entered in the same step, it is not possible to know how each variable affected the relation between ADHD and digital media use.
Effects of rater
As mentioned in the method section, all studies but three used ratings to assess ADHD symptom levels and/or digital media use. A majority of the studies also used the same rater for both the predictor and the outcome measure, with 11 studies using only self-ratings and 8 studies using only parent ratings. Associations can be over-estimated if the same rater is used to assess both the predictor and the outcome, and the validity of youth self-reports of ADHD symptom levels can also be questioned. We therefore conducted additional sensitivity analyses to determine whether results differed depending on what type of rater that was used. The results showed that there were no systematic differences between studies reporting significant and non-significant associations with regard to whether the study used parent ratings, self-ratings, or a combination of raters.”
Discussion
The aim of the present review was to summarize findings from longitudinal studies published during the past 10 years that have addressed the association between digital media use and ADHD symptoms. We found 28 studies meeting our inclusion criteria: 10 addressed reciprocal relations between digital media use and ADHD symptoms, 9 addressed only the association between digital media use and later ADHD symptoms, and 9 addressed only the association between ADHD symptoms and later digital media. The present results showed that a majority (74%) of the studies found significant associations between digital media and later ADHD symptom levels. Effects sizes were often relatively small (e.g., correlation coefficients < 0.30). However, as discussed further below, even small associations may be of importance when controlling for baseline levels in longitudinal studies. In addition, the present review found at least partial support for reciprocal associations, suggesting that ADHD symptoms are related to an increased risk of developing problematic use of digital media, which in turn can exaggerate both their symptom levels and daily life problems due to both the directs effects (e.g., multitasking, quick rewards) and the indirect effects (e.g., negative effects on sleep and social relations) of digital media. In the discussion below, we point to some important limitations of previous research that should be addressed in future studies aimed at better understanding the complex relations between digital media use and ADHD symptoms.
Factors to take into consideration when interpreting the results
Generally, both the associations between digital media use and later ADHD symptoms and the reverse associations were relatively small. This could be taken to indicate that digital media use and ADHD are not strongly linked. However, there are several important aspects to take into consideration when interpreting the results of the present review. First, it should be noted that the size of the associations depended on what type of digital media that was in focus. In the present review, eight of the nine studies investigating digital media addiction found some significant associations, whereas effects were less consistently found when examining screen time. This could indicate that it is primarily when digital media use has negative consequences for daily life functioning that it is associated with ADHD symptom levels. However, we believe that parents need to monitor their child’s digital media use carefully as early prevention is important and parents play a vital role in teaching children how to use digital media in a balanced way [69, 70].
Second, it has been argued [71] that when controlling for baseline levels in longitudinal studies, even small associations should be considered meaningful when there is high stability in the outcome variable. In the studies included in this review, correlations between ADHD symptom levels at different time-points were high and substantially higher compared to correlations between digital media across time-points. Thus, when investigating relations between digital media and later ADHD symptom levels and controlling for baseline ADHD symptom levels, there is relatively little variance left to explain.
A third issue relates to differential associations. As will be discussed in more detail below, few of the examined studies investigated the role of moderators. Thus, the relatively small associations referred to above apply to the average associations for the entire sample. However, there are likely subgroups of children with ADHD who are at relatively high risk of developing digital media addiction and identifying this “at-risk” group should be of high priority for future research.
A fourth important issue to consider when assessing the size of effects is the time lag between baseline and follow-up. Some digital media effects can have immediate consequences (e.g., cyberbullying or sexual harassment), whereas other effects (e.g., multitasking, playing games with high arousal) take considerably longer to manifest themselves. Many studies included in the present review covered a time span of 1–2 years, which may seem sensible. However, it is possible that some associations might have been missed, because the time span was too short or that the main part of the effect occurred shortly after use began and then remained stable.
A fifth issue concerns the use of more advanced statistical methods that can reveal to what extent associations can only be found for between-subject effects (i.e., how average media use across many children are related to the average ADHD symptom levels of the same children) or whether there is also evidence of within-subject effects (i.e., child X’s media use is related to child X’s ADHD symptoms across time). Only four studies included in the present review investigated both these two types of associations, and two of these studies also found support for within-subject associations. Another important statistical issue relates to control for baseline levels in the outcome measure. In the summary of the results presented in Fig. 2, we demonstrated that results varied substantially based on what type of analyses that were conducted. When interpreting the results of the present review, it should therefore be important to take into consideration that only a small minority of the studies conducted within-subject analyses, which is the type of analysis that provides the strongest support for causal associations.
Even when conducting within-subject analyses, we need to be careful to not interpret the results of the longitudinal studies included in this review as necessarily providing evidence of causal relations. It is possible that associations are driven by other variables, not included in the studies, which are related to both digital media and ADHD symptom levels. Although the study by McNamee et al. [45] showed that associations remained significant when including many different covariates and running several different types of sensitivity analyses, this is an issue that needs to be further addressed in future research.
Finally, it should be noted that only two studies included in the present review investigated non-linear relations. Although, both these studies [40, 45] failed to find evidence of non-linear relations between digital media use and later ADHD symptoms, there are strong reasons to believe that a certain level of digital media use is needed to produce negative effects. By focusing only on linear associations, effects might be underestimated. A previous meta-analysis [72] even found that moderate use of digital media (i.e., less than 2 h/day) was related to lower levels of mental health problems compared to no digital media use at all, while the reverse was true for more excessive use. As using digital media has become the norm in today’s society, not using digital media at all, or not being allowed to use certain games or mobile applications commonly used by the child’s peers, might even have negative effects on peer relations and mental health.
Direction of associations
One of the great advantages of longitudinal studies is that they can inform us about the direction of the associations. In analyses controlling for baseline levels, the present review found support for a significant relation between digital media and later ADHD symptoms in 12 of 19 (63%) studies and support for the reverse relation in 10 of 19 (53%) studies. However, the best design for studies investigating the direction of associations is of course to look at bi-directional relations (i.e., how digital media and ADHD symptoms mutually influence each other over time). In the ten studies using this design, bi-directional relations were found in only 3 of 10 (30%) studies. In the remaining studies, four studies found support for a relation between digital media use and later ADHD symptoms (i.e., media effects rather than selection effects), two studies found support for the reverse relation, and the last study did not find any significant relations. When interpreting these results, there are some methodological issues that need to be considered. As discussed above, measures of ADHD symptoms are more highly correlated across time compared to digital media use, making it more difficult to find an association between digital media use and later ADHD symptoms compared to the reverse effect [4]. As discussed briefly above, the issue of the time lag between baseline and follow-up is also important to consider, especially in studies investigating bi-directional associations. If selection effects (i.e., ADHD in relation to later digital media) take longer or shorter to manifest themselves compared to media effects (i.e., digital media in relation to later ADHD symptoms), a fixed time lag cannot take this into consideration, possibly resulting in an underestimation of some associations. Effects of ADHD in relation to later digital media use most likely take some time to manifest themselves. With regard to effects of digital media use on later ADHD symptoms, it has been argued that some direct effects, such as those of violent media, are apparent quickly [4], whereas effects of, for example, multitasking [47] take longer. In conclusion, there seems to be relatively strong support for an association between digital media use and later ADHD symptoms as well as vice versa. However, more longitudinal studies examining reciprocal associations are needed, as we were only able to locate ten such studies and these studies showed mixed findings.
Moderators, mediators and covariates
As concerns sex differences, the present study did not focus on main differences with regard to digital media use or ADHD, but rather on to what extent the associations between digital media use and later ADHD symptoms or vice versa are stronger for one sex compared to the other. Unfortunately, the present review does not shed much light on this issue due to the limited number of studies using sex as a moderator. However, one study found support for a stronger association between violent media and ADHD symptoms among boys [50], and another study found some support for a stronger association between media multitasking and ADHD symptoms among girls [47]. These findings may seem contradictory at first, but they are most likely related to the fact that Baumgarten et al. [47] investigated media multitasking (i.e., an activity more common among girls), whereas Rydell and Brocki [50] investigated screen time for violent media (i.e., an activity more common among boys), and interaction effects are more easily detected in samples with a large range in the variables of interests. However, we would like to emphasize that the significant interaction effects of sex were small and that another study included in the review [56] failed to find a significant moderating effect of sex, suggesting that sex is not a very important moderator in the association between digital media use and ADHD.
As concerns age, the studies included in the present review included children from 18 months to 17 years. Significant associations were found in some studies of younger children [48, 49], but not in other studies looking at children of a similar age [58]. The results were mixed in studies of older children and adolescents as well. Because adolescence is a period of substantial restructuring of the brain, it has been argued to be an especially sensitive period, also regarding the influences of digital media use [73]. Early adolescence is also the period during which many children begin using digital media to a much greater extent than previously, with some official statistics [e.g., 74] showing that “age 13 is the new 16” (i.e., that digital media use now peaks already at age 13 compared to the previous peak at 16 years). Some support for this notion was found in the present review, as Baumgarten et al. [47] found associations between digital multitasking and ADHD symptoms for younger but not older adolescents. In addition, some have argued that effects should instead be the greatest in preschool children, owing to the rapid cognitive and socioemotional development that takes place during this period in life, and research has shown that early screen time does have effects on cognition [e.g., 75], externalizing behaviors [76] and attentional networks in the brain [77]. Interestingly, previous research has found associations even when infants are only exposed to a TV in the background [e.g., 78] or when parents are disrupted by their digital media devices when interacting with their preschool child [e.g., 79].
Regarding additional moderators and mediators, Barlett et al. [53] showed that digital media use was associated with sleep problems, which in turn was associated with increased ADHD symptom levels. Their results are in line with previous studies demonstrating a link between sleep and both digital media use [32] and ADHD [80]. Somewhat surprisingly, we found no longitudinal studies investigating the mediating role of neuropsychological functions, such as executive functions (i.e., working memory, inhibitory control, and planning), delay aversion and emotion regulation, given that these functions have been linked to digital media use [81,82,83], other types of additions such as alcohol/drug addiction or gambling [84, 85], and ADHD [86]. Given that ADHD is a highly heterogeneous disorder, it is important that future research both identify subgroups with the highest risk of developing digital media addiction and better adapt treatment to meet the needs of individual patients.
Directions for future research
Although we believe that the present review provides important information, there are some important aspects that require further investigation. First, associations often became non-significant when different covariates were included, which indicates that at least some of these factors are of importance for the association between digital media use and ADHD symptoms. However, rather than including a large range of variables simultaneously, their role as potential mediators or moderators in the relation between digital media use and ADHD symptoms needs to be investigated. We recommend that multiple mediation/moderation models, which promote a better understanding of the complex associations between digital media use and ADHD, be used. Second, we need to move away from investigating only screen time or symptoms of digital media addiction and focus on what type of media use is most problematic and what media activities might even promote positive development. Some of the studies included in the present review did not aim to specifically investigate associations between digital media and ADHD symptom levels, and this was just briefly assessed within a larger study with a much broader aim. To obtain more detailed information, future studies also need to include more precise measurements. As emphasized previously [87], using several types of measures in the same study should also be considered important, as different measures have different strengths and weaknesses. We recommend that future research uses new technological advancements to obtain more detailed information on what type of digital media content children encounter and how this contributes to later mental health outcomes. One study included in the present review [57] provided some insights into this issue by showing that the types of media activities with the highest odds ratios in relation to ADHD symptom levels were video chatting, playing games with yourself, and online shopping/browsing. The lowest odds ratio was found for sending text messages.
Third, we need more longitudinal studies investigating effects of social media in relation to ADHD symptom levels. Although a few studies included in the present review examined Internet addiction (i.e., a combined measure of all types of digital media activities), only two of them [45, 46] focused specifically on social media.
Fourth, we need to use measures other than ratings and use different raters for the predictor and the outcome. Only three reports included in the present review [40,41,42] used interviews to assess digital media addiction and/or ADHD symptom levels, and this should clearly be considered an important strength of these studies. It should also be noted that the quality criteria indicated that only eight studies used different raters for the predictor and the outcome, which means that associations might have been over-estimated due to rater biases.
Fifth, it is also important to emphasize that longitudinal studies such as those included in the current review need to be complemented with studies using experimental designs to obtain more detailed information about factors that trigger and maintain a problematic use of digital media in children with ADHD. Finally, none of the studies in the present review included clinically referred samples of children diagnosed with ADHD, and this should be considered an important avenue for future longitudinal research.
Clinical relevance and implications
The results of the present review support the “Differential susceptibility to media effects model” [24], which states that some individuals are more vulnerable to developing problematic use of digital media. Some support was also found for the “Reciprocal Spirals Model” [10], which states that digital media and ADHD have reciprocal effects across time, meaning that using digital media when you have ADHD can result in increased symptom levels over time. As described in the present introduction, it has been hypothesized that excessive digital media use can also cause a range of displacement effects, such as low levels of physical activity, sleep problems, and poor eating habits. Because these lifestyle factors are associated with ADHD, we believe that it is important for clinicians to discuss digital media habits as one potential factor contributing to both increased ADHD symptom levels and exacerbated daily life problems. It should also be noted that once unhealthy life habits have been formed, they are very difficult to change. Thus, parents of children with ADHD need to be aware that their children are at higher risk of being attracted to digital media and that there are characteristics found in many types of digital media (both games and social media) that are more rewarding for children with ADHD, making these children more prone to developing addiction problems. In addition, extensive use of digital media can exacerbate ADHD symptom levels as well as comorbid problems, both directly due to the characteristics of the media (e.g., violent content, fast pace, multitasking, and quick rewards) and indirectly through the negative effects digital media use has on, for example, academic achievement and social relations. Recommendations for digital media use for children have been developed [e.g., 88] and they often include no screen time at all for children under the age of 2, 1–2 h of only high-quality media between age 2–5, and consistent limits even for older children, the goal being to ensure that digital media use does not have negative effects. Importantly, previous research [e.g., 89, 90] has shown that, in many countries, the average screen time for children greatly exceeds these limits, with averages continuously increasing and families with low SES being less likely to follow recommendations. Thus, it is necessary to work actively with parents, schools, and the healthcare sector to promote greater awareness and support children at-risk of developing digital media addiction. During the past few years, politicians and authorities in several countries have also begun discussing the need for new legislation that will force the tech industry to exclude game characteristics that are particularly addictive or detrimental to mental health. These characteristics include infinite scrolling, autoplay, rewarding users for merely using their services, and photo filters that encourage unhealthy beauty ideals [e.g., 91, 92]. In-game purchasing of loot-boxes is another feature that has been shown to have severe negative consequences for children (e.g., stealing from parents or putting oneself in debt), and the Gambling Health Alliance in the UK [93] has therefore suggested that loot-boxes be banned in games for children. Regardless of whether legislation or mutual discussions with the tech industry are the best way forward, we welcome both more research on and political discussions of how to reduce the harmful effects of digital media use on children.
Finally, we like to acknowledge that the conclusions from this review could open up for speculations of a future differential diagnosis such as “digital media induced ADHD” and rightfully raise concerns of potential consequences thereof (e.g., stigma, validity of the ADHD diagnosis, and right to treatment). We would therefore like to emphasize the need for future studies to investigate such issues with more complex methodology, investigating the impact and role of other explanatory factors (moderating and mediating effects). To what extent digital media can cause an ADHD diagnosis is not what this review has investigated as all included studies investigated ADHD symptom levels (i.e., hyperactivity, impulsivity, and inattention) without taking the other diagnostic criteria for ADHD into account.
Conclusions
The present review shows that digital media use is related to later ADHD as well as vice versa. Thus, these associations are best characterized as reciprocal, in that digital media and ADHD symptom levels affect each other in a complex relation over time. Even though these associations are sometimes small, they should be regarded as important, because they are found rather consistently across studies. Due to the fact that ADHD symptom levels are highly correlated across time, there is also little variance left to explain when investigating digital media in relation to later ADHD symptom levels and controlling for ADHD symptoms at baseline. The present review further shows that associations with ADHD appear stronger for longitudinal studies investigating problematic use of digital media compared to those focusing on screen time. Associations do not appear to be strongly related to either the age or sex of the child. However, the fact that some relations did not remain significant when including covariates could be taken to indicate that there are certain subgroups of children with ADHD symptoms that are more vulnerable to the effects of digital media. Conducting both moderation and mediation analyses should be an important avenue for future longitudinal research if we are to identify subgroups as well as underlying factors that can better explain the link between digital media use and ADHD symptom levels.
Availability of data and materials
No applicable.
Code availability
Not applicable.
References
vom Orde H, Durner A (2020). International Data on Youth and Media 2020. International Central Institute for Youth and Educational Television. https://www.br-online.de/jugend/izi/english/International%20Data%20on%20Youth%20and%20Media.pdf. Accessed 3 Aug 2022
OECD (2019). PISA 2018 Results (Volume III): What School Life Means for Students’ Lives; PISA. OECD Publishing. https://www.oecd-ilibrary.org///sites/acd78851-en/1/2/12/index.html?itemId=/content/publication/acd78851-en&_csp_=34b83bd6f1788b01629355b271dcc687&itemIGO=oecd&itemContentType=book#s83. Accessed 3 Aug 2022
Xu G, Strathearn L, Liu B, Yang B, Bao W (2018) Twenty-year trends in diagnosed attention-deficit/hyperactivity disorder among US children and adolescents, 1997–2016. JAMA Netw Open 1(4):e181471. https://doi.org/10.1001/jamanetworkopen.2018.1471
Beyens I, Valkenburg PM, Piotrowski JT (2018) Screen media use and ADHD-related behaviors: four decades of research. Proc Natl Acad Sci U S A 115(40):9875–9881. https://doi.org/10.1073/pnas.1611611114
Engelhard MM, Kollins SH (2019) The many channels of screen media technology in ADHD: a paradigm for quantifying distinct risks and potential benefits. Curr Psychiatry Rep 21(9):90. https://doi.org/10.1007/s11920-019-1077-1
Ferguson CJ (2015) Do angry birds make for angry children? A meta-analysis of video game influences on children’s and adolescents’ aggression, mental health, prosocial behavior, and academic performance. Perspect Psychol Sci 10(5):646–666. https://doi.org/10.1177/1745691615592234
Kuss DJ, Griffiths MD (2012) Internet gaming addiction: a systematic review of empirical research. Int J Ment Health Addict 10(2):278–296. https://doi.org/10.1007/s11469-011-9318-5
Ho RC, Zhang MWB, Tsang TY et al (2014) The association between Internet addiction and psychiatric co-morbidity: a meta-analysis. BMC Psychiatry 14:183. https://doi.org/10.1186/1471-244X-14-183
Wang B-Q, Yao N-Q, Zhou X, Liu J, Lv Z-T (2017) The association between attention deficit/hyperactivity disorder and Internet addiction: a systematic review and meta-analysis. BMC Psychiatry. https://doi.org/10.1186/s12888-017-1408-x
Slater MD (2015) Reinforcing spirals model: conceptualizing the relationship between media content exposure and the development and maintenance of attitudes. Media Psychol 18(3):370–395. https://doi.org/10.1080/15213269.2014.897236
WHO (2018). International Statistical Classification of Diseases and Related Health Problems (11th Revision). World Health Organization
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5). 5th ed. American Psychiatric Association Publishing
Andreassen CS (2015) Online social network site addiction: a comprehensive review. Curr Addict Rep 2(2):175–184. https://doi.org/10.1007/s40429-015-0056-9
Bányai F, Zsila Á, Király O et al (2017) Problematic social media use: results from a large-scale nationally representative adolescent sample. PLoS One 12(1):e0169839. https://doi.org/10.1371/journal.pone.0169839
van den Eijnden RJJM, Lemmens JS, Valkenburg PM (2016) The social media disorder scale. Comput Human Behav 61:478–487. https://doi.org/10.1016/j.chb.2016.03.038
Burén J, Nutley SB, Sandberg D, Ström Wiman J, Thorell LB (2021) Gaming and social media addiction in university students: sex differences, suitability of symptoms, and association with psychosocial difficulties. Front Psychiatry 12:740867. https://doi.org/10.3389/fpsyt.2021.740867
Paschke K, Austermann MI, Thomasius R (2021) ICD-11-based assessment of social media use disorder in adolescents: development and validation of the social media use disorder scale for adolescents. Front Psychiatry 12:661483. https://doi.org/10.3389/fpsyt.2021.661483
Wong HY, Mo HY, Potenza MN et al (2020) Relationships between severity of Internet gaming disorder, severity of problematic social media use, sleep quality and psychological distress. Int J Environ Res Public Health 17(6):1879. https://doi.org/10.3390/ijerph17061879
Zendle D, Bowden-Jones H (2019) Is excessive use of social media an addiction? BMJ 365:l2171. https://doi.org/10.1136/bmj.l2171
Jensen PS, Mrazek D, Knapp PK et al (1997) Evolution and revolution in child psychiatry: ADHD as a disorder of adaptation. J Am Acad Child Adolesc Psychiatry 36(12):1672–1679. https://doi.org/10.1097/00004583-199712000-00015. (discussion 1679-81)
Christakis DA, Zimmerman FJ, DiGiuseppe DL, McCarty CA (2004) Early television exposure and subsequent attentional problems in children. Pediatrics 113(4):708–713. https://doi.org/10.1542/peds.113.4.708
Nikkelen SWC, Valkenburg PM, Huizinga M, Bushman BJ (2014) Media use and ADHD-related behaviors in children and adolescents: a meta-analysis. Dev Psychol 50(9):2228–2241. https://doi.org/10.1037/a0037318
Madore KP, Khazenzon AM, Backes CW et al (2020) Memory failure predicted by attention lapsing and media multitasking. Nature 587(7832):87–91. https://doi.org/10.1038/s41586-020-2870-z
Valkenburg PM, Peter J (2013) The differential susceptibility to media effects model: differential susceptibility to media effects model. J Commun 63(2):221–243. https://doi.org/10.1111/jcom.12024
Marco R, Miranda A, Schlotz W et al (2009) Delay and reward choice in ADHD: an experimental test of the role of delay aversion. Neuropsychology 23(3):367–380. https://doi.org/10.1037/a0014914
Hoza B (2007) Peer functioning in children with ADHD. Ambul Pediatr 7(1):101–106. https://doi.org/10.1016/j.ambp.2006.04.011
Daley D, Birchwood J (2010) ADHD and academic performance: why does ADHD impact on academic performance and what can be done to support ADHD children in the classroom?: ADHD and academic performance. Child Care Health Dev 36(4):455–464. https://doi.org/10.1111/j.1365-2214.2009.01046.x
Melodia F, Canale N, Griffiths MD (2020) The role of avoidance coping and escape motives in problematic online gaming: a systematic literature review. Int J Ment Health Addiction. https://doi.org/10.1007/s11469-020-00422-w
Zywica J, Danowski J (2008) The faces of facebookers: Investigating social enhancement and social compensation hypotheses; Predicting facebook™ and offline popularity from sociability and self-esteem, and mapping the meanings of popularity with semantic networks. J Comput Mediat Commun 14(1):1–34. https://doi.org/10.1111/j.1083-6101.2008.01429.x
Pearson N, Braithwaite RE, Biddle SJ, van Sluijs EM, Atkin AJ (2014) Associations between sedentary behaviour and physical activity in children and adolescents: a meta-analysis. Obes Rev 15(8):666–675. https://doi.org/10.1111/obr.12188
Saunders TJ, McIsaac T, Douillette K et al (2020) Sedentary behaviour and health in adults: an overview of systematic reviews. Appl Physiol Nutr Metab 45(10; Suppl. 2):S197–S217. https://doi.org/10.1139/apnm-2020-0272
Hale L, Guan S (2015) Screen time and sleep among school-aged children and adolescents: a systematic literature review. Sleep Med Rev 21:50–58. https://doi.org/10.1016/j.smrv.2014.07.007
Twenge JM, Spitzberg BH, Campbell WK (2019) Less in-person social interaction with peers among U.S. adolescents in the 21st century and links to loneliness. J Soc Pers Relat 36(6):1892–1913. https://doi.org/10.1177/0265407519836170
Madigan S, McArthur BA, Anhorn C, Eirich R, Christakis DA (2020) Associations between screen use and child language skills: a systematic review and meta-analysis. JAMA Pediatr 174(7):665–675. https://doi.org/10.1001/jamapediatrics.2020.0327
Holton KF, Nigg JT (2020) The association of lifestyle factors and ADHD in children. J Atten Disord 24(11):1511–1520. https://doi.org/10.1177/1087054716646452
Carli V, Durkee T, Wasserman D et al (2013) The association between pathological Internet use and comorbid psychopathology: a systematic review. Psychopathology 46(1):1–13. https://doi.org/10.1159/000337971
Karaca S, Saleh A, Canan F, Potenza MN (2017) Comorbidity between behavioral addictions and attention deficit/hyperactivity disorder: a systematic review. Int J Ment Health Addict 15(3):701–724. https://doi.org/10.1007/s11469-016-9660-8
Suchert V, Hanewinkel R, Isensee B (2015) Sedentary behavior and indicators of mental health in school-aged children and adolescents: a systematic review. Prev Med 76:48–57. https://doi.org/10.1016/j.ypmed.2015.03.026
Page MJ, McKenzie JE, Bossuyt PM et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Stenseng F, Hygen BW, Wichstrøm L (2020) Time spent gaming and psychiatric symptoms in childhood: cross-sectional associations and longitudinal effects. Eur Child Adolesc Psychiatry 29(6):839–847. https://doi.org/10.1007/s00787-019-01398-2
Wichstrøm L, Stenseng F, Belsky J, von Soest T, Hygen BW (2019) Symptoms of Internet gaming disorder in youth: predictors and comorbidity. J Abnorm Child Psychol 47(1):71–83. https://doi.org/10.1007/s10802-018-0422-x
Hygen BW, Skalická V, Stenseng F, Belsky J, Steinsbekk S, Wichstrøm L (2020) The co-occurrence between symptoms of Internet gaming disorder and psychiatric disorders in childhood and adolescence: prospective relations or common causes? J Child Psychol Psychiatry 61(8):890–898. https://doi.org/10.1111/jcpp.13289
National Institutes of Health. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. Study Quality Assessment Tools (2013). https://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools/cohort. Accessed 9 Aug 2021
Beyens I, Piotrowski JT, Valkenburg PM (2020) Which came first? Assessing transactional relationships between children’s violent media use and ADHD-related behaviors. Communic Res 47(8):1228–1245. https://doi.org/10.1177/0093650218782300
McNamee P, Mendolia S, Yerokhin O (2021) Social media use and emotional and behavioural outcomes in adolescence: evidence from British longitudinal data. Econ Hum Biol 41:100992. https://doi.org/10.1016/j.ehb.2021.100992
Boer M, Stevens G, Finkenauer C, van den Eijnden R (2020) Attention deficit hyperactivity disorder-symptoms, social media use intensity, and social media use problems in adolescents: investigating directionality. Child Dev 91(4):e853–e865. https://doi.org/10.1111/cdev.13334
Baumgartner SE, van der Schuur WA, Lemmens JS, te Poel F (2018) The relationship between media multitasking and attention problems in adolescents: results of two longitudinal studies: Media multitasking and attention problems. Hum Commun Res 44(1):3–30. https://doi.org/10.1111/hcre.12111
Hetherington E, McDonald S, Racine N, Tough S (2020) Longitudinal predictors of self-regulation at school entry: findings from the all our families cohort. Children. https://doi.org/10.3390/children7100186
Liu W, Wu X, Huang K et al (2021) Early childhood screen time as a predictor of emotional and behavioral problems in children at 4 years: a birth cohort study in China. Environ Health Prev Med 26(1):3. https://doi.org/10.1186/s12199-020-00926-w
Rydell A-M, Brocki KC (2021) ADHD symptoms and callous-unemotional traits as predictors of violent media use in adolescence. Scand J Psychol 62(1):25–33. https://doi.org/10.1111/sjop.12693
Männikkö N, Ruotsalainen H, Miettunen J, Kääriäinen M (2020) Associations between childhood and adolescent emotional and behavioral characteristics and screen time of adolescents. Issues Ment Health Nurs 41(8):700–712. https://doi.org/10.1080/01612840.2020.1725195
Allen MS, Vella SA (2015) Screen-based sedentary behaviour and psychosocial well-being in childhood: cross-sectional and longitudinal associations. Ment Health Phys Act 9:41–47. https://doi.org/10.1016/j.mhpa.2015.10.002
Barlett ND, Gentile DA, Barlett CP, Eisenmann JC, Walsh DA (2012) Sleep as a mediator of screen time effects on us children’s health outcomes: a prospective study. J Child Media 6(1):37–50. https://doi.org/10.1080/17482798.2011.633404
Gentile DA, Swing EL, Lim CG, Khoo A (2012) Video game playing, attention problems, and impulsiveness: evidence of bidirectional causality. Psychol Pop Media Cult 1(1):62–70. https://doi.org/10.1037/a0026969
Parkes A, Sweeting H, Wight D, Henderson M (2013) Do television and electronic games predict children’s psychosocial adjustment? Longitudinal research using the UK Millennium Cohort Study. Arch Dis Child 98(5):341–348. https://doi.org/10.1136/archdischild-2011-301508
Poulain T, Vogel M, Neef M et al (2018) Reciprocal associations between electronic media use and behavioral difficulties in preschoolers. Int J Environ Res Public Health 15(4):814. https://doi.org/10.3390/ijerph15040814
Ra CK, Cho J, Stone MD et al (2018) Association of digital media use with subsequent symptoms of attention-deficit/hyperactivity disorder among adolescents. JAMA 320(3):255. https://doi.org/10.1001/jama.2018.8931
Niiranen J, Kiviruusu O, Vornanen R, Saarenpää-Heikkilä O, Paavonen EJ (2021) High-dose electronic media use in five-year-olds and its association with their psychosocial symptoms: a cohort study. BMJ Open 11(3):e040848. https://doi.org/10.1136/bmjopen-2020-040848
Poulain T, Vogel M, Ludwig J, Grafe N, Körner A, Kiess W (2019) Reciprocal longitudinal associations between adolescents’ media consumption and psychological health. Acad Pediatr 19(1):109–117. https://doi.org/10.1016/j.acap.2018.08.009
Ferguson CJ, Wang CKJ (2021) Aggressive video games are not a risk factor for mental health problems in youth: a longitudinal study. Cyberpsychol Behav Soc Netw 24(1):70–73. https://doi.org/10.1089/cyber.2020.0027
Wartberg L, Kriston L, Zieglmeier M, Lincoln T, Kammerl R (2019) A longitudinal study on psychosocial causes and consequences of Internet gaming disorder in adolescence. Psychol Med 49(2):287–294. https://doi.org/10.1017/S003329171800082X
Ferguson CJ, Ceranoglu TA (2014) Attention problems and pathological gaming: resolving the “chicken and egg” in a prospective analysis. Psychiatr Q 85(1):103–110. https://doi.org/10.1007/s11126-013-9276-0
Chen Y-L, Chen S-H, Gau SS-F (2015) ADHD and autistic traits, family function, parenting style, and social adjustment for Internet addiction among children and adolescents in Taiwan: a longitudinal study. Res Dev Disabil 39:20–31. https://doi.org/10.1016/j.ridd.2014.12.025
Yang SJ, Stewart R, Lee JY et al (2014) Prevalence and correlates of problematic Internet experiences and computer-using time: a two-year longitudinal study in korean school children. Psychiatry Investig 11(1):24–31. https://doi.org/10.4306/pi.2014.11.1.24
Jeong H, Yim HW, Lee S-Y et al (2020) Low self-control and aggression exert serial mediation between inattention/hyperactivity problems and severity of Internet gaming disorder features longitudinally among adolescents. J Behav Addict 9(2):401–409. https://doi.org/10.1556/2006.2020.00039
Peeters M, Koning I, van den Eijnden R (2018) Predicting Internet gaming disorder symptoms in young adolescents: a one-year follow-up study. Comput Human Behav 80:255–261. https://doi.org/10.1016/j.chb.2017.11.008
Wartberg L, Zieglmeier M, Kammerl R (2021) An empirical exploration of longitudinal predictors for problematic Internet use and problematic gaming behavior. Psychol Rep 124(2):543–554. https://doi.org/10.1177/0033294120913488
Hirota T, Takahashi M, Adachi M, Sakamoto Y, Nakamura K (2021) Neurodevelopmental traits and longitudinal transition patterns in Internet addiction: a 2-year prospective study. J Autism Dev Disord 51(4):1365–1374. https://doi.org/10.1007/s10803-020-04620-2
Bender PK, Kim EL, Gentile DA (2020) Gaming disorder in children and adolescents: risk factors and preventive approaches. Curr Addict Rep 7:553–560. https://doi.org/10.1007/s40429-020-00337-5
Bonnaire C, Liddle HA, Har A, Nielsen P, Phan O (2019) Why and how to include parents in the treatment of adolescents presenting Internet gaming disorder? J Behav Addict 8(2):201–212. https://doi.org/10.1556/2006.8.2019.27
Adachi P, Willoughby T (2015) Interpreting effect sizes when controlling for stability effects in longitudinal autoregressive models: implications for psychological science. Eur J Dev Psychol 12(1):116–128. https://doi.org/10.1080/17405629.2014.963549
Liu M, Wu L, Yao S (2016) Dose-response association of screen time-based sedentary behaviour in children and adolescents and depression: a meta-analysis of observational studies. Br J Sports Med 50(20):1252–1258. https://doi.org/10.1136/bjsports-2015-095084
Crone EA, Konijn EA (2018) Media use and brain development during adolescence. Nat Commun 9(1):1–10. https://doi.org/10.1038/s41467-018-03126-x
Swedish Media Council (2019). Ungar & Medier. https://statensmedierad.se/publikationer/ungarochmedier/ungarochmedier2019.3347.html. Accessed 3 Aug 2022
Tomopoulos S, Dreyer BP, Berkule S, Fierman AH, Brockmeyer C, Mendelsohn AL (2010) Infant media exposure and toddler development. Arch Pediatr Adolesc Med 164(12):1105–1111. https://doi.org/10.1001/archpediatrics.2010.235
McNeill J, Howard SJ, Vella SA, Cliff DP (2019) Longitudinal associations of electronic application use and media program viewing with cognitive and psychosocial development in preschoolers. Acad Pediatr 19(5):520–528. https://doi.org/10.1016/j.acap.2019.02.010
Zivan M, Bar S, Jing X, Hutton J, Farah R, Horowitz-Kraus T (2019) Screen-exposure and altered brain activation related to attention in preschool children: an EEG study. Trends Neurosci Educ 17:100117. https://doi.org/10.1016/j.tine.2019.100117
Schmidt ME, Pempek TA, Kirkorian HL, Lund AF, Anderson DR (2008) The effects of background television on the toy play behavior of very young children. Child Dev 79(4):1137–1151. https://doi.org/10.1111/j.1467-8624.2008.01180.x
Sundqvist A, Heimann M, Koch F-S (2020) Relationship between family technoference and behavior problems in children aged 4–5 years. Cyberpsychol Behav Soc Netw 23(6):371–376. https://doi.org/10.1089/cyber.2019.0512
Sung V, Hiscock H, Sciberras E, Efron D (2008) Sleep problems in children with attention-deficit/hyperactivity disorder: prevalence and the effect on the child and family. Arch Pediatr Adolesc Med 162(4):336–342. https://doi.org/10.1001/archpedi.162.4.336
Argyriou E, Davison CB, Lee TTC (2017) Response inhibition and Internet gaming disorder: a meta-analysis. Addict Behav 71:54–60. https://doi.org/10.1016/j.addbeh.2017.02.026
Ioannidis K, Hook R, Goudriaan AE et al (2019) Cognitive deficits in problematic Internet use: meta-analysis of 40 studies. Br J Psychiatry 215(5):639–646. https://doi.org/10.1192/bjp.2019.3
Marino C, Caselli G, Lenzi M et al (2019) Emotion regulation and desire thinking as predictors of problematic Facebook use. Psychiatr Q 90(2):405–411. https://doi.org/10.1007/s11126-019-09628-1
Jovanovski D, Erb S, Zakzanis KK (2005) Neurocognitive deficits in cocaine users: a quantitative review of the evidence. J Clin Exp Neuropsychol 27(2):189–204. https://doi.org/10.1080/13803390490515694
MacKillop J, Amlung MT, Few LR, Ray LA, Sweet LH, Munafò MR (2011) Delayed reward discounting and addictive behavior: a meta-analysis. Psychopharmacology 216(3):305–321. https://doi.org/10.1007/s00213-011-2229-0
Castellanos FX, Sonuga-Barke EJ, Milham MP, Tannock R (2006) Characterizing cognition in ADHD: beyond executive dysfunction. Trends Cogn Sci 10(3):117–123. https://doi.org/10.1016/j.tics.2006.01.011
Vandewater EA, Lee SJ (2009) Measuring children’s media use in the digital age: issues and challenges. Am Behav Sci 52(8):1152–1176. https://doi.org/10.1177/0002764209331539
World Health Organization (2019). Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age
Radesky JS, Christakis DA (2016) Increased screen time: implications for early childhood development and behavior. Pediatr Clin North Am 63:827–839. https://doi.org/10.1016/j.pcl.2016.06.006
Määttä S, Konttinen H, Haukkala A, Erkkola M, Roos E (2017) Preschool children’s context-specific sedentary behaviours and parental socioeconomic status in Finland: a cross-sectional study. BMJ Open 7(11):e016690. https://doi.org/10.1136/bmjopen-2017-016690
Griffiths MD, Nuyens F (2017) An overview of structural characteristics in problematic video game playing. Curr Addict Rep 4:272–283. https://doi.org/10.1007/s40429-017-0162-y
Montag C, Lachmann B, Herrlich M, Zweig K (2019) Addictive features of social media/messenger platforms and freemium games against the background of psychological and economic theories. Int J Environ Res Public Health 16(14):2612. https://doi.org/10.3390/ijerph16142612
The Royal College of Paediatrics and Child Health. (2019) The Health Impacts of Screen Time: A Guide for Clinicians and Parents. https://www.rcpch.ac.uk/sites/default/files/2018-12/rcpch_screen_time_guide_-_final.pdf. Accessed 3 Aug 2022
Funding
Open access funding provided by Karolinska Institute. The present study was supported by a grant to the first author from the Swedish Research Council for Health, Working Life and Welfare (Forte).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no relevant financial or non-financial interests to disclose.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Thorell, L.B., Burén, J., Ström Wiman, J. et al. Longitudinal associations between digital media use and ADHD symptoms in children and adolescents: a systematic literature review. Eur Child Adolesc Psychiatry (2022). https://doi.org/10.1007/s00787-022-02130-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00787-022-02130-3