
Poor Adherence to the WHO Guidelines on Feeding Practices Increases the Risk for Respiratory Infections in Surinamese Preschool Children

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
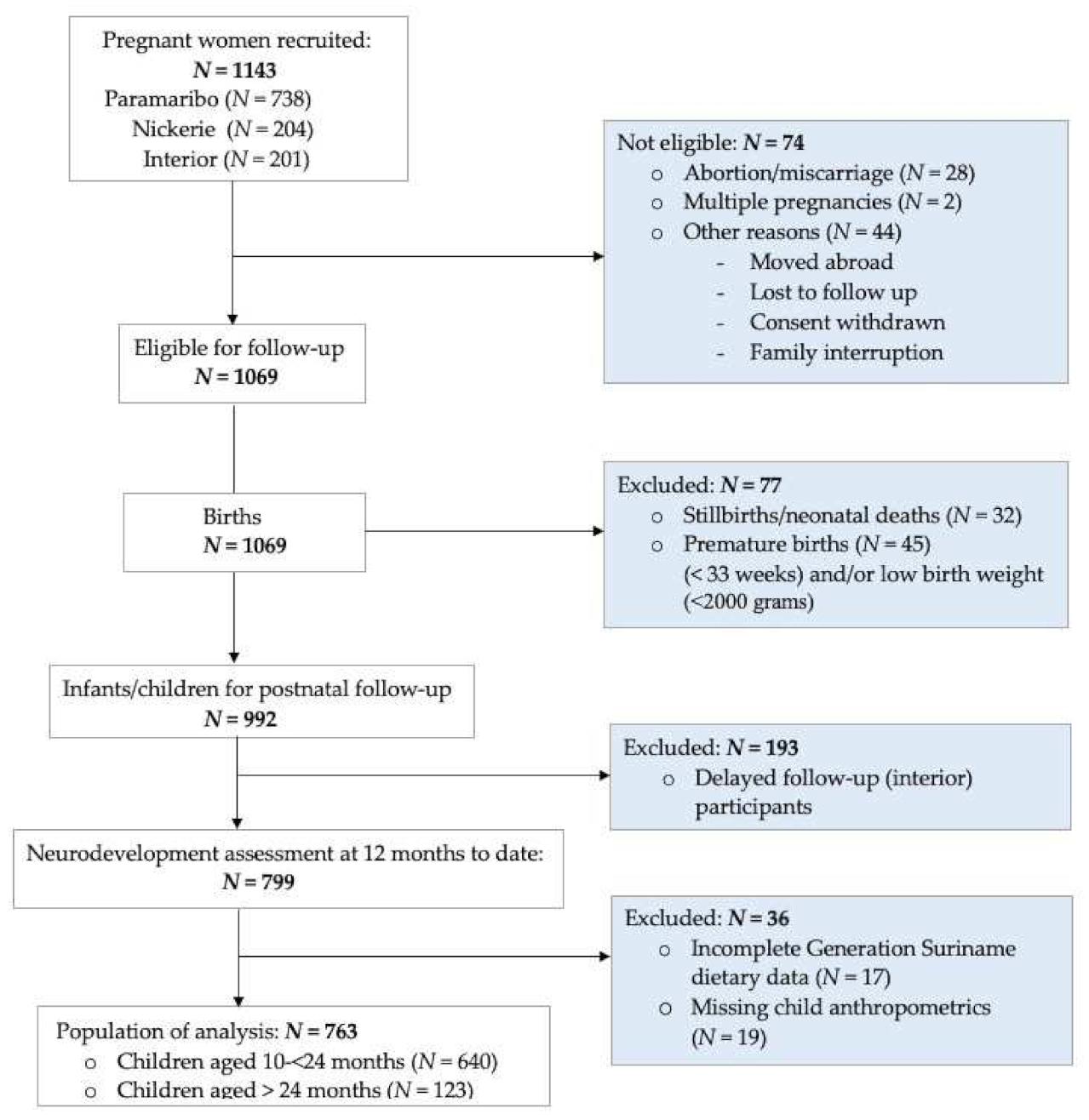
2.1. Study Design and Study Population
2.2. Feeding Indicators
- MDD: this indicator was considered achieved when receiving foods from at least four out of the six food groups [24];
- MMF: the minimum requirement was defined as four times per day for breastfed infants and five times (three meals with two additional snacks) per day for non-breastfed children aged ≥ 24 months [25];
- MAD: this composite indicator was considered achieved when the MDD and MMF indicators were met.
2.3. Infant Characteristics
2.4. Maternal Demographics
2.5. Respiratory Tract Infection
2.6. Statistical Analyses
2.7. IYCF Indicators
2.8. Associations between Feeding Practices and Respiratory Health Effects
- Currently breastfed;
- Child characteristics: birth weight, gender;
- Food allergies;
- Maternal characteristics: age, educational level, ethnicity, parity;
- Maternal characteristics: household income and marital status.
2.9. Ethical Considerations
3. Results
3.1. Population Characteristics
3.2. Assessment of Respiratory Tract Infections
3.2.1. Upper or Lower Respiratory Tract Infections
3.2.2. Upper Respiratory Tract Infections
3.2.3. Lower Respiratory Tract Infections
3.3. Feeding Practices and Respiratory Tract Infections
3.3.1. IYCF Practices and Upper Respiratory Tract Infections
3.3.2. IYCF Practices and Lower Tract Infections
3.3.3. Complementary Feeding Practices According to Place of Residence
Children < 24 Months of Age
Children ≥ 24 Months of Age
4. Discussion
4.1. Association between Respiratory Tract Infections and IYCF Indicators Children (10–33) Months in Suriname
4.2. IYCF Indicators According to Place of Residence
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Predictors | Upper RTI | * Lower RTI | Upper or Lower RTI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | |
| Model 1:MDD/MMF MDD Parity Household income |
0.53 0.64 | [0.38, 0.76] [0.43, 0.96] | <0.001 0.03 | 0.77 | [0.62,0.96] | 0.02 | 0.51 0.65 | [0.36, 0.72] [0.43, 0.98] | <0.001 0.04 |
| Model 2: MAD MAD Parity Household income | 0.55 0.63 | [0.39, 0.78] [0.42, 0.94] | <0.001 0.03 | 0.77 | [0.62, 0.97] | 0.03 |
0.55 0.64 |
[0.39, 0.77] [0.43, 0.96] | <0.001 0.03 |
Appendix B
| Place of Residence | P 1 | N 2 | I 3 | |
|---|---|---|---|---|
| IYCF Indicators | ||||
| Achieved MDD | P I | |||
| Achieved MMF | I | I | ||
| Achieved MAD | I | P I | ||
References
- United Nations Inter-Agency Group for Child Mortality Estimation (UN IGME). Levels & Trends in Child Mortality: Report 2020, Estimates Developed by the United Nations Inter-Agency Group for Child Mortality Estimation; United Nations Children’s Fund: New York, NY, USA, 2020. [Google Scholar]
- United Nations Inter-Agency Group for Child Mortality Estimation. CME Info-Child Mortality Estimates. 2020. Available online: https://childmortality.org/data (accessed on 18 April 2021).
- Suriname (SUR)—Demographics, Health & Infant Mortality—UNICEF DATA. 2019. Available online: https://data.unicef.org/country/sur/ (accessed on 17 April 2021).
- Goodarzi, E.; Sohrabivafa, M.; Darvishi, I.; Naemi, H.; Khazaei, Z. Epidemiology of mortality induced by acute respiratory infections in infants and children under the age of 5 years and its relationship with the Human Development Index in Asia: An updated ecological study. J. Public Health 2021, 29, 1047–1054. [Google Scholar] [CrossRef]
- Black, R.E.; Cousens, S.; Johnson, H.L.; Lawn, J.; Rudan, I.; Bassani, D.; Jha, P.; Campbell, H.; Walker, C.F.; Cibulskis, R.; et al. Global, regional, and national causes of child mortality in 2008: A systematic analysis. Lancet 2010, 375, 1969–1987. [Google Scholar] [CrossRef]
- Rudan, I.; Tomaskovic, L.; Boschi-Pinto, C.; Campbell, H. Global estimate of the incidence of clinical pneumonia among children under five years of age. Bull. World Health Organ. 2004, 82, 895–903. [Google Scholar]
- Ujunwa, F.; Ezeonu, C. Risk Factors for Acute Respiratory Tract Infections in Under-five Children in Enugu Southeast Nigeria. Ann. Med. Health Sci. Res. 2014, 4, 95–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Global Nutrition Report Action on Equity to End Malnutrition; WHO: Bristol, UK, 2020. [Google Scholar]
- Mazumdar, S. Determinants of inequality in child malnutrition in India. Asian Popul. Stud. 2010, 6, 307–333. [Google Scholar] [CrossRef]
- Van de Poel, E.; Hosseinpoor, A.R.; Speybroeck, N.; Van Ourti, T.; Vega, J. Socioeconomic inequality in malnutrition in developing countries. Bull. World Health Organ. 2008, 86, 282–291. [Google Scholar] [CrossRef] [Green Version]
- Morais, A.H.D.A.; Aquino, J.D.S.; da Silva-Maia, J.K.; Vale, S.H.D.L.; Maciel, B.L.L.; Passos, T.S. Nutritional status, diet and viral respiratory infections: Perspectives for severe acute respiratory syndrome coronavirus 2. Br. J. Nutr. 2021, 125, 851–862. [Google Scholar] [CrossRef] [PubMed]
- AboElfotoh, M.N.; Rasheed, E.M.; Sharaf, S.M.; Tohamy, N.A.B. Evaluation of Nutritional Status of Children with Acute Lower Respiratory Tract Infection. Egypt. J. Hosp. Med. 2020, 79, 532–537. [Google Scholar] [CrossRef]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Grant, C.C.; Wall, C.R.; Gibbons, M.J.; Morton, S.M.; Santosham, M.; Black, R.E. Child nutrition and lower respiratory tract disease burden in New Zealand: A global context for a national perspective. J. Paediatr. Child Health 2011, 47, 497–504. [Google Scholar] [CrossRef]
- Stewart, C.P.; Iannotti, L.; Dewey, K.G.; Michaelsen, K.F.; Onyango, A.W. Contextualising complementary feeding in a broader framework for stunting prevention. Matern. Child Nutr. 2013, 9, 27–45. [Google Scholar] [CrossRef]
- Rodríguez, L.; Cervantes, E.; Ortiz, R. Malnutrition and Gastrointestinal and Respiratory Infections in Children: A Public Health Problem. Int. J. Environ. Res. Public Health 2011, 8, 1174–1205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, A.L.; Sacco, L.; Hyder, A.; Black, R. Malnutrition as an underlying cause of childhood deaths associated with infectious diseases in developing countries. Bull. World Health Organ. 2000, 78, 1207–1221. [Google Scholar] [PubMed]
- Global Nutrition Report Suriname| Country Nutrition Profiles—Global Nutrition Report. Available online: https://globalnutritionreport.org/resources/nutrition-profiles/latin-america-and-caribbean/south-america/suriname/ (accessed on 30 August 2021).
- WHO; UNICEF; USAID; AED; UCDAVIS. Indicators for Assessing Infant and Young Child Feeding Practices: Part 1: Definitions; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Minstry of Social Affairs and, Housing, and General Bureau of Statistics. Suriname Multiple Indicator Cluster Survey 2010, Final Report. 2012. Available online: https://www.statistics-suriname.org/wp-content/uploads/2019/02/suriname-mics4-2010-complete-with-cover.pdf (accessed on 23 November 2020).
- Zijlmans, W.; Wickliffe, J.; Hindori-Mohangoo, A.; MacDonald-Ottevanger, S.; Ouboter, P.; Landburg, G.; Codrington, J.; Roosblad, J.; Baldewsingh, G.; Ramjatan, R.; et al. Caribbean Consortium for Research in Environmental and Occupational Health (CCREOH) Cohort Study: Influences of complex environmental exposures on maternal and child health in Suriname. BMJ Open 2020, 10, e034702. [Google Scholar] [CrossRef] [PubMed]
- Jaddoe, V.W.V.; Van Duijn, C.M.; Van Der Heijden, A.J.; MacKenbach, J.P.; Moll, H.A.; Steegers, E.A.P.; Tiemeier, H.; Uitterlinden, A.G.; Verhulst, F.C.; Hofman, A. The Generation R Study: Design and cohort update 2010. Eur. J. Epidemiol. 2010, 25, 823–841. [Google Scholar] [CrossRef] [PubMed]
- WHO; UNICEF; USAID; AED; UCDAVIS; IFPRI; WHO. Indicators for Assessing Infant and Young Child Feeding Practices. Part 2 Measurement; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Do, B.T.; Hansen, N.I.; Bann, C.; Lander, R.L.; Goudar, S.S.; Pasha, O.; Chomba, E.; Dhaded, S.M.; Thorsten, V.R.; Wallander, J.L.; et al. Associations between feeding practices and growth and neurodevelopmental outcomes at 36 months among children living in low- and low-middle income countries who participated in the BRAIN-HIT trial. BMC Nutr. 2018, 4, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Handbook: IMCI Integrated Management of Childhood Illness; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Tromp, I.; Kiefte-de Jong, J.; Raat, H.; Jaddoe, V.; Franco, O.; Hofman, A.; de Jongste, J.; Moll, H. Breastfeeding and the risk of respiratory tract infections after infancy: The Generation R Study. PLoS ONE 2017, 12, e0172763. [Google Scholar] [CrossRef] [Green Version]
- Duijts, L.; Jaddoe, V.W.V.; Hofman, A.; Moll, H.A. Prolonged and Exclusive Breastfeeding Reduces the Risk of Infectious Diseases in Infancy. Pediatrics 2010, 126, e18–e25. [Google Scholar] [CrossRef] [Green Version]
- Tromp, I.I.; Jong, J.C.K.-D.; de Vries, J.H.; Jaddoe, V.W.; Raat, H.; Hofman, A.; de Jongste, J.C.; Moll, H.A. Dietary patterns and respiratory symptoms in pre-school children: The Generation R Study. Eur. Respir. J. 2012, 40, 681–689. [Google Scholar] [CrossRef] [Green Version]
- Chatzi, L.; Kogevinas, M. Prenatal and childhood Mediterranean diet and the development of asthma and allergies in children. Public Health Nutr. 2009, 12, 1629–1634. [Google Scholar] [CrossRef]
- Arimond, M.; Torheim, L.E.; Wiesmann, D.; Joseph, M.; Carriquiry, A. Dietary Diversity as a Measure of the Micronutrient Adequacy of Women’s Diets: Results from Rural Bangladesh Site; Food and Nutrition Technical Assistance II Project, Academy for Educational Development: Washington, DC, USA, 2000. [Google Scholar]
- Venter, C.; Greenhawt, M.; Meyer, R.W.; Agostoni, C.; Reese, I.; Du Toit, G.; Feeney, M.; Maslin, K.; Nwaru, B.I.; Roduit, C.; et al. EAACI position paper on diet diversity in pregnancy, infancy and childhood: Novel concepts and implications for studies in allergy and asthma. Allergy 2020, 75, 497–523. [Google Scholar] [CrossRef] [Green Version]
- Steyn, N.P.; Nel, J.H.; Nantel, G.; Kennedy, G.; Labadarios, D. Food variety and dietary diversity scores in children: Are they good indicators of dietary adequacy? Public Health Nutr. 2006, 9, 644–650. [Google Scholar] [CrossRef] [Green Version]
- Rathnayake, K.M.; Madushani, P.; Silva, K.R. Use of dietary diversity score as a proxy indicator of nutrient adequacy of rural elderly people in Sri Lanka. BMC Res. Notes 2012, 5, 469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khamis, A.G.; Mwanri, A.W.; Ntwenya, J.E.; Kreppel, K. The influence of dietary diversity on the nutritional status of children between 6 and 23 months of age in Tanzania. BMC Pediatr. 2019, 19, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caulfield, L.E.; De Onis, M.; Blössner, M.; Black, R. Undernutrition as an underlying cause of child deaths associated with diarrhea, pneumonia, malaria, and measles. Am. J. Clin. Nutr. 2004, 80, 193–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paoli, A.; Tinsley, G.; Bianco, A.; Moro, T. The Influence of Meal Frequency and Timing on Health in Humans: The Role of Fasting. Nutrients 2019, 11, 719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO; PAN. Guiding Principles for Feeding Non-Breastfed Children 6–24 Months of Age; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; De Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J.; Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Shah, P.S.; Knowledge Synthesis Group on Determinants of LBW/PT Births. Parity and low birth weight and preterm birth: A systematic review and meta-analyses. Acta Obstet. Gynecol. Scand. 2010, 89, 862–875. [Google Scholar] [CrossRef]
- Gaillard, R.; Rurangirwa, A.A.; Williams, M.A.; Hofman, A.; Mackenbach, J.P.; Franco, O.; Steegers, E.A.; Jaddoe, V.W. Maternal Parity, Fetal and Childhood Growth, and Cardiometabolic Risk Factors. Hypertension 2014, 64, 266–274. [Google Scholar] [CrossRef] [Green Version]
- Koullali, B.; Van Zijl, M.D.; Kazemier, B.M.; Oudijk, M.A.; Mol, B.W.J.; Pajkrt, E.; Ravelli, A.C.J. The association between parity and spontaneous preterm birth: A population based study. BMC Pregnancy Childbirth 2020, 20, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Simonsen, S.M.E.; Lyon, J.L.; Alder, S.C.; Varner, M.W. Effect of Grand Multiparity on Intrapartum and Newborn Complications in Young Women. Obstet. Gynecol. 2005, 106, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Aina-Mumuney, A.J.; Rai, K.K.; Taylor, M.Y.; Weitz, C.M.; Chisholm, C.A. Nulliparity and Duration of Pregnancy in Multiple Gestation. Obstet. Gynecol. 2004, 104, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Steiner, L.; Diesner, S.C.; Voitl, P. Risk of infection in the first year of life in preterm children: An Austrian observational study. PLoS ONE 2019, 14, e0224766. [Google Scholar] [CrossRef]
- Ray, K.N.; Lorch, S.A. Hospitalization of Early Preterm, Late Preterm, and Term Infants During the First Year of Life by Gestational Age. Hosp. Pediatr. 2013, 3, 194–203. [Google Scholar] [CrossRef] [Green Version]
- Miller, J.E.; Hammond, G.C.; Strunk, T.; Moore, H.C.; Leonard, H.; Carter, K.W.; Bhutta, Z.; Stanley, F.; De Klerk, N.; Burgner, D. Association of gestational age and growth measures at birth with infection-related admissions to hospital throughout childhood: A population-based, data-linkage study from Western Australia. Lancet Infect. Dis. 2016, 16, 952–961. [Google Scholar] [CrossRef] [Green Version]
- Epps, T.W.; Salkind, N. Omnibus Tests. In Encyclopedia of Research Design; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Faber, J.; Fonseca, L.M. How sample size influences research outcomes. Dent. Press J. Orthod. 2014, 19, 27–29. [Google Scholar] [CrossRef]
- Getrouw, A.; Hindori-Mohangoo, A.; Zijlmans, W.; Mans, D. Ethnic Differences in Breastfeeding Initiation and Duration among Mothers Attending Primary Healthcare Clinics in Paramaribo, Suriname. West Indian Med. J. 2017. [Google Scholar] [CrossRef] [Green Version]

| Total (N = 763) Respiratory Tract Infections | Not Achieved MDD 1 (N = 367) | Achieved MDD (N = 393) | p-Value | Not Achieved MMF (N = 88) | Achieved MMF (N = 675) | p-Value | Not Achieved MAD 1 (N = 396) | Achieved MAD (N = 364) | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | |||
| URTI 547 (71.7) | 287 (78.2) | 257 (65.4) | <0.001 * | 64 (72.7) | 483 (71.6) | 0.82 | 306 (77.3) | 238 (65.4) | <0.001 * |
| LRTI 97 (12.7) | 50 (13.6) | 45 (11.5) | 0.37 | 13 (14.8) | 84 (12.4) | 0.54 | 52 (13.1) | 43 (11.8) | 0.58 |
| RTI 554 (72.6) | 292 (79.6) | 262 (66.7) | <0.001 * | 65 (73.9) | 492 (72.9) | 0.85 | 311 (78.5) | 243 (66.8) | <0.001 * |
| Predictors | URTI | LRTI | RTI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | OR | 95% CI | β | OR | 95% CI | β | OR | 95% CI | |
| (Constant) | 2.61 | 13.64 | −3.28 | 0.04 | 2.61 | 13.60 | |||
| Model 1 | |||||||||
| MDD | −0.62 | 0.53 | 0.38, 0.76 * | −0.15 | 0.86 | 0.53,1.37 | −0.65 | 0.52 | 0.37, 0.74 * |
| MMF | 0.05 | 0.95 | 0.53, 1.71 | 0.28 | 1.33 | 0.60, 2.91 | −0.02 | 0.98 | 0.54, 1.77 |
| Cumulatively adjusted for | |||||||||
| currently breastfed (0 = not breastfed) | −0.13 | 0.88 | 0.59, 1.31 | 0.04 | 1.04 | 0.61, 1.78 | −0.15 | 86 | 0.58, 1.29 |
| Cumulatively adjusted for | |||||||||
| birth weight (in grams) | 0.00 | 1.00 | 0.99, 1.00 | 0.00 | 1.00 | 1.0, 1.0 | 0.00 | 1.00 | 0.99, 1.00 |
| gender (0 = female) | 0.13 | 1.13 | 0.81, 1.59 | 0.21 | 1.23 | 0.77, 1.96 | 0.15 | 1.16 | 0.83, 1.63 |
| Cumulatively adjusted for | |||||||||
| food allergies (0 = no) | 0.23 | 1.26 | 0.55, 2.89 | 0.45 | 1.57 | 0.60, 4.08 | 0.14 | 1.15 | 0.49, 2.66 |
| Cumulatively adjusted for | |||||||||
| Maternale age (in years) | −0.01 | 0.99 | 0.96, 1.02 | 0.03 | 1.03 | 0.99, 1.07 | −0.01 | 0.99 | 0.96, 1.02 |
| Educational level | 0.09 | 1.09 | 0.87, 1.36 | 0.02 | 1.03 | 0.75, 1.39 | 0.12 | 1.12 | 0.89, 1.40 |
| (ref = no or primary level) | |||||||||
| Parity (0 = primi) | −0.45 | 0.64 | 0.43, 0.96 * | 0.08 | 1.08 | 0.61, 1.89 | −0.43 | 0.65 | 0.43, 0.98 * |
| Maternal ethnicity (ref = mixed) | |||||||||
| (Creole) | 0.12 | 1.13 | 0.62, 2.06 | 0.34 | 1.4 | 0.60, 3.27 | 0.11 | 1.11 | 0.60, 2.06 |
| (Hindustani) | 0.013 | 1.01 | 0.75, 1.80 | −0.09 | 0.92 | 0.38, 2.20 | −0.08 | 0.92 | 0.51, 1.65 |
| (Indigenous) | 0.181 | 1.20 | 0.58, 2.49 | 0.59 | 1.80 | 0.68, 4.75 | 0.19 | 1.21 | 0.57, 2.56 |
| (Javanese) | 0.01 | 1.01 | 0.50, 2.05 | 0.23 | 1.26 | 0.46, 3.42 | −0.04 | 0.96 | 0.47, 1.97 |
| (Tribal) | 0.03 | 1.04 | 0.55, 1.95 | −0.66 | 0.52 | 0.19, 1.39 | −0.06 | 0.94 | 0.49, 1.79 |
| Cumulatively adjusted for Marital status | |||||||||
| (ref = not married/living with partner) | −0.28 | 0.76 | 0.43, 1.34 | 0.18 | 0.1.20 | 0.55, 2.60 | −0.25 | 0.78 | 0.44, 1.34 |
| Household income (in SRD) | −0.05 | 0.95 | 0.81, 1.11 | −0.26 | 0.77 | 0.62, 0.96 * | −0.08 | 0.92 | 0.79, 1.08 |
| Predictors | URTI | LRTI | RTI | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | OR | 95 % CI | β | OR | 95% CI | β | OR | 95% CI | |
| (Constant) | 2.60 | 13.40 | −3.07 | 0.05 | 2.61 | 13.60 | |||
| Model 2 | |||||||||
| MAD | −0.59 | 0.55 | 0.39, 0.78 * | 0.02 | 0.86 | 0.53,1.37 | −0.60 | 0.55 | 0.37, 0.74 * |
| Adjusted for currently breastfed | −0.16 | 0.85 | 0.58, 1.25 | 0.01 | 1.01 | 0.60, 1.72 | −0.19 | 83 | 0.58, 1.29 |
| (0 = not breastfed) | |||||||||
| Cumulatively adjusted for | |||||||||
| birth weight (in grams) | 0.00 | 1.00 | 0.99, 1.00 | 0.00 | 1.00 | 1.0, 1.0 | 0.00 | 1.00 | 0.99, 1.00 |
| gender (0 = female) | 0.11 | 1.11 | 0.80, 1.57 | 0.20 | 1.23 | 0.77, 1.95 | 0.14 | 1.15 | 0.81, 1.61 |
| Cumulatively adjusted for | |||||||||
| food allergies (0 = no) | 0.20 | 1.22 | 0.53, 2.81 | 0.44 | 1.55 | 0.60, 4.04 | 0.11 | 1.12 | 0.49, 2.57 |
| Cumulatively adjusted for | |||||||||
| Maternale age (in years) | −0.01 | 0.99 | 0.96, 1.02 | 0.02 | 1.03 | 0.99, 1.07 | −0.01 | 0.99 | 0.96, 1.02 |
| Educational level | 0.09 | 1.09 | 0.88, 1.36 | 0.03 | 1.03 | 0.76, 1.40 | 0.12 | 1.12 | 0.90, 1.40 |
| (ref = no or primary level) | |||||||||
| Parity (0 = primi) | −0.46 | 0.63 | 0.42, 0.94 * | 0.07 | 1.07 | 0.61, 1.89 | −0.45 | 0.64 | 0.43, 0.96 * |
| Maternal ethnicity (ref = mixed) | |||||||||
| (Creole) | 0.15 | 1.16 | 0.64, 2.12 | 0.37 | 1.4 | 0.62, 3.36 | 0.14 | 1.15 | 0.63, 2.12 |
| (Hindustani) | 0.03 | 1.03 | 0.58, 1.84 | −0.08 | 0.92 | 0.38, 2.20 | −0.06 | 0.94 | 0.53, 1.69 |
| (Indigenous) | 0.19 | 1.21 | 0.59, 2.52 | 0.55 | 1.80 | 0.66, 4.58 | 0.20 | 1.22 | 0.58, 2.58 |
| (Javanese) | 0.02 | 1.02 | 0.50, 2.07 | 0.23 | 1.26 | 0.46, 3.43 | −0.03 | 0.97 | 0.47, 1.99 |
| (Tribal) | 0.07 | 1.08 | 0.58, 2.02 | −0.66 | 0.52 | 0.19, 1.39 | −0.02 | 0.98 | 0.52, 1.86 |
| Marital status | −0.29 | 0.75 | 0.42, 1.32 | 0.18 | 0.1.20 | 0.55, 2.59 | −0.26 | 0.77 | 0.44, 1.38 |
| (ref = not married/living with partner) | |||||||||
| Household income (in SRD) | −0.04 | 0.96 | 0.81, 1.12 | −0.25 | 0.77 | 0.62, 0.96 * | −0.07 | 0.93 | 0.79, 1.08 |
| Place of Residence | Place of Residence | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (N = 586) | Overall Practice (95% CI) | <24 Months (N = 481) | P (N = 224) | N (N = 142) | I (N = 115) | p-Value | ≥24 Months (N = 105) | P (N = 59) | N (N = 30) | I (N = 16) | p-Value |
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | ||
| Achieved MDD 1 N = 315 (53.7) | (50.0–58.0) | 250 (52.3) | 112 (50.0) | 96 (67.6) | 42 (36.5) | <0.001 * | 65 (61.9) | 33 (55.9) | 23 (76.7) | 9 (56.3) | 0.14 |
| Achieved MMF N = 503 (85.8) | (82.8–88.4) | 412 (87.7) | 211 (94.2) | 132 (93.0) | 69 (60.0) | <0.001 * | 91 (86.7) | 52 (88.1) | 27 (90.0) | 2 (75.0) | 0.32 |
| Achieved MAD 1 N = 289 (49.3) | (45.5–53.6) | 230 (47.8) | 107 (47.8) | 89 (62.7) | 34 (29.6) | <0.001 * | 59 (56.2) | 31 (52.5) | 20 (66.7) | 8 (50.0) | 0.39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wormer, J.R.; Shankar, A.; Van Hensbroek, M.B.; Hindori-Mohangoo, A.D.; Covert, H.; Lichtveld, M.Y.; Zijlmans, W.C.W.R. Poor Adherence to the WHO Guidelines on Feeding Practices Increases the Risk for Respiratory Infections in Surinamese Preschool Children. Int. J. Environ. Res. Public Health 2021, 18, 10739. https://doi.org/10.3390/ijerph182010739
Wormer JR, Shankar A, Van Hensbroek MB, Hindori-Mohangoo AD, Covert H, Lichtveld MY, Zijlmans WCWR. Poor Adherence to the WHO Guidelines on Feeding Practices Increases the Risk for Respiratory Infections in Surinamese Preschool Children. International Journal of Environmental Research and Public Health. 2021; 18(20):10739. https://doi.org/10.3390/ijerph182010739
Chicago/Turabian StyleWormer, Jill R., Arti Shankar, Michael Boele Van Hensbroek, Ashna D. Hindori-Mohangoo, Hannah Covert, Maureen Y. Lichtveld, and Wilco C. W. R. Zijlmans. 2021. "Poor Adherence to the WHO Guidelines on Feeding Practices Increases the Risk for Respiratory Infections in Surinamese Preschool Children" International Journal of Environmental Research and Public Health 18, no. 20: 10739. https://doi.org/10.3390/ijerph182010739